
The micronutrient essential for brain health that 90 percent of people don't get enough of
What choline does for the aging brain, how much you need, why it is hard to test, the foods that supply it, the APOE4 angle, and when a supplement makes sense
Last week I went through the drugs and substances that affect dementia risk, and one class carried the most safety signal of any. The anticholinergics, the medications that block acetylcholine, showed the most consistent association with dementia across the evidence, with a clear dose-response pattern. Acetylcholine is the chemical messenger the brain relies on for memory and attention, and those drugs work by interfering with it.
The approved cholinergic Alzheimer’s drugs do the opposite of those anticholinergics. The three cholinesterase inhibitors, donepezil, rivastigmine, and galantamine, block the enzyme that breaks down acetylcholine and raise its availability at brain receptors, and they remain the standard symptomatic treatment even though the clinical benefit is relatively small (review).
The other side of that same pathway is choline, the nutrient the brain uses to build acetylcholine in the first place. It does not get the attention that protein or omega-3s do, and most people take in less than the recommended amount without realizing it. According to the NIH Office of Dietary Supplements, the average adult intake is about 402 mg per day in men and 278 mg per day in women, under the targets of 550 and 425 mg. Around 90 percent of adults come up short.
That gap matters because choline sits behind two of the brain’s basic operations.
Why choline matters for the aging brain
The two jobs. Choline is a building block for phosphatidylcholine and sphingomyelin, the fatty molecules that form the membranes around every neuron, and it is the raw material the body uses to make acetylcholine, the signaling chemical tied to memory and attention (NIH ODS). The liver makes a small amount of choline on its own, but not enough, which is why diet has to cover the rest.
The deficiency signal. When choline runs low, the first organ to show it is the liver, because phosphatidylcholine is needed to package and export fat. In controlled feeding studies, adults placed on a low-choline diet developed measurable liver dysfunction that reversed once choline was restored (Fischer and colleagues, 2007). The brain effects are slower and harder to see, which is part of why choline gets overlooked.
Why APOE4 carriers may have a higher choline requirement
What APOE4 is. APOE (apolipoprotein E) is a gene that codes for a protein that ferries cholesterol and other fats around the body and the brain. It comes in three common versions, APOE2, APOE3, and APOE4, and each person inherits one copy from each parent. The APOE4 version is the strongest common inherited risk factor for late-onset Alzheimer’s. Carrying one copy raises lifetime risk roughly two to threefold and carrying two copies raises it around tenfold, while about a quarter of people carry at least one copy. It shifts risk rather than fixing an outcome, and a large part of that risk runs through metabolic and blood-vessel pathways that diet and lifestyle can influence. I carry one copy of APOE4 myself, which is part of why I follow this research closely, and I have written more about what carrying it means in my article on APOE4.
The finding. Work from the lab of Dr. Li-Huei Tsai at MIT gives a specific reason a carrier might need more choline. In human brain cells engineered to carry the APOE4 gene, the cells mishandled fats and accumulated lipid droplets, and adding choline reversed much of that defect by feeding phospholipid synthesis (Sienski and colleagues, 2021). The interpretation was that APOE2 and APOE3 cells cope with mild choline shortage while APOE4 cells have a harder time.
The mouse support. In mice bred to develop Alzheimer-like changes, lifelong choline supplementation lowered amyloid plaque load and improved memory, with reduced inflammatory activation of the brain’s immune cells, in work from Dr. Ramon Velazquez and Dr. Salvador Oddo (Velazquez and colleagues, 2019).
The human test. The genotype-targeted study this calls for has only been done at a small scale so far, a 15-person Phase 1 trial in APOE4 carriers measuring fat-handling markers in spinal fluid rather than memory. It is one of several promising leads, not a settled answer, and a larger trial would be needed before the APOE4 supplementation idea could be called proven. I placed choline in the low-risk, mechanism-based tier for carriers in my earlier review of nootropics and neurorestoratives graded by the evidence.
How dietary choline tracks with dementia risk
The U-shape. A large dietary study drawing on more than 125,000 UK Biobank participants found that the relationship between choline intake and dementia is U-shaped (Yuan and colleagues, 2024). People in the second-lowest quartile of intake, around 330 to 350 mg per day, had lower dementia and Alzheimer’s risk than those in the lowest quartile, while the lowest and highest intakes carried more risk. Earlier cohorts including Framingham pointed the same direction, linking higher choline to better memory and less small-vessel brain damage (Poly and colleagues, 2011). That low point sits below the Adequate Intake of 425 and 550 mg, but the two numbers measure different things, since the intake target is a deficiency floor set to protect the liver while the dementia curve simply bottomed out a bit lower. Because the bottom of that curve is broad and dietary intake is estimated imprecisely, meeting the higher target lands close to the lowest-risk range rather than working against it.
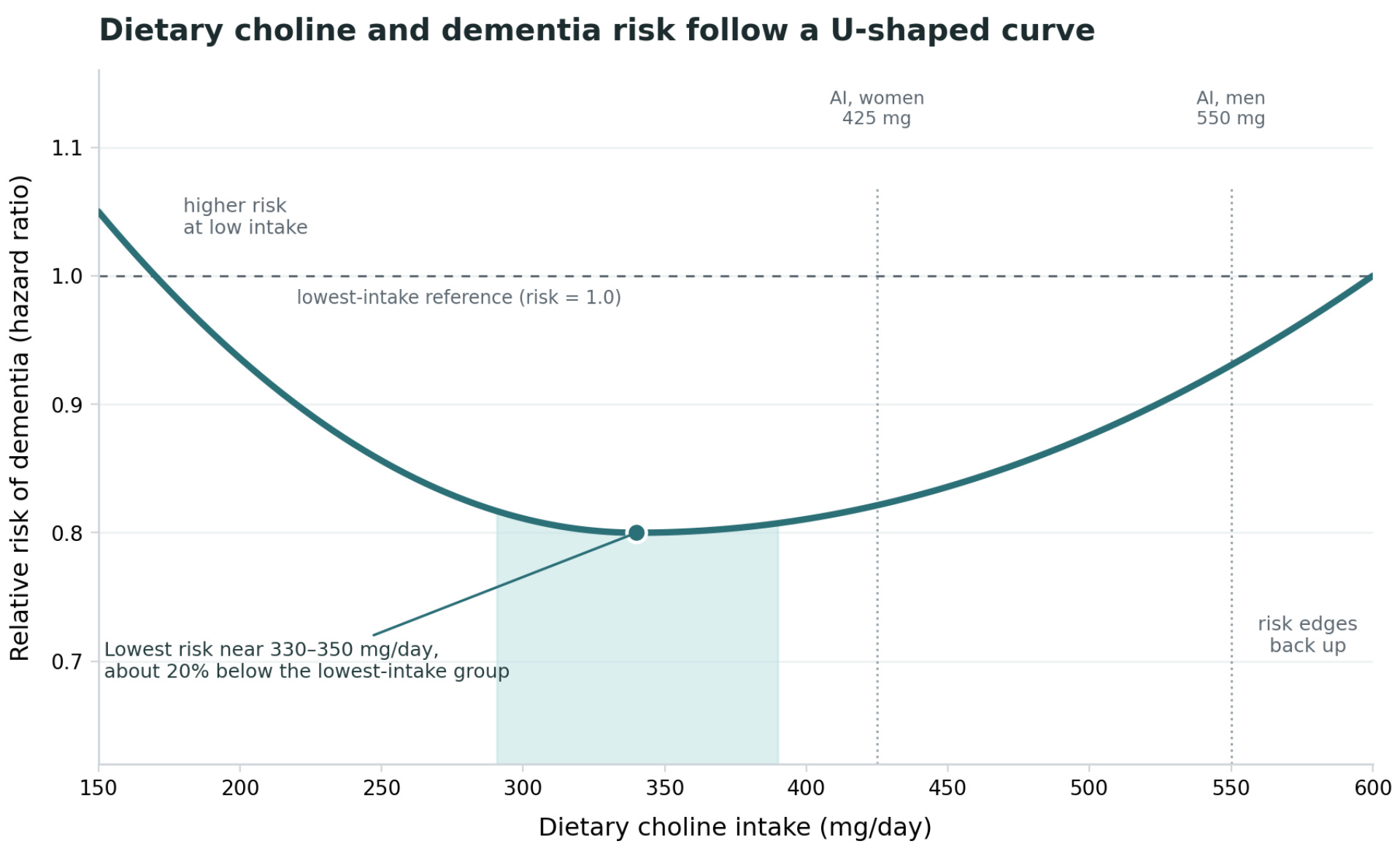
The ceiling. The upper arm of that U is the reason more is not automatically better. Excess choline that the gut cannot absorb gets converted by gut bacteria into trimethylamine N-oxide, or TMAO, a substance that has been linked to cardiovascular risk. The practical reading is that a moderate, consistent intake looks better than a maximal one.
Which foods supply the most choline
Animal foods tend to carry more choline per serving, with eggs as the main contributor in the typical diet, though some plants help. The values below come from the USDA database compiled by the NIH.
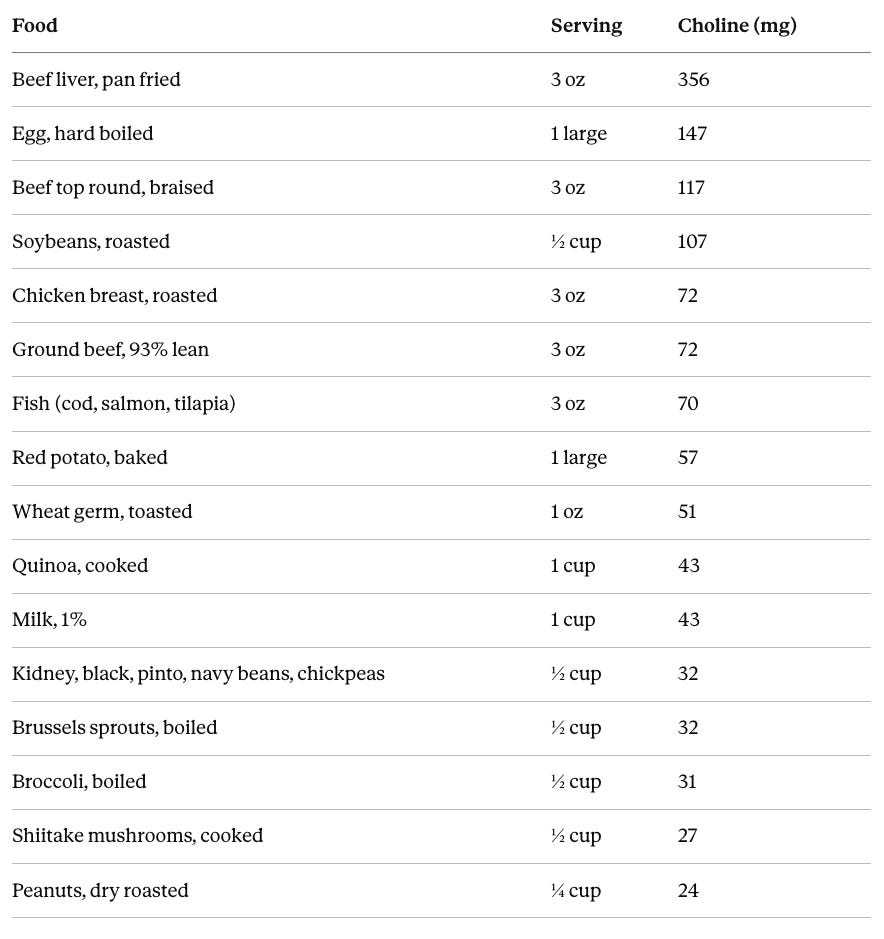
Red meat and especially processed red meat carry choline but also carry their own higher dementia and cardiovascular risk, so eggs, fish, poultry, and legumes are the lower-risk way to reach the target (Li and colleagues, 2025).
What a normal day of choline adds up to
The math. Two eggs supply close to 294 mg, which already covers most of a day for a woman and more than half for a man. Add a 3 oz serving of chicken, fish, or lean beef for another 70 mg or so, plus a half cup of beans or soybeans and a serving of cruciferous vegetables, and a normal day clears 400 to 500 mg without much effort. A single serving of beef liver covers an entire day on its own, which is part of why liver shows up so often in older nutrition advice.
A note on the cholesterol question. The old one-egg-a-day rule came from a 300 mg daily cholesterol ceiling that United States guidelines recommended for decades, and that ceiling was dropped in the 2015 to 2020 Dietary Guidelines for Americans (review). Most pooled studies find no clear cardiovascular risk from up to one egg a day in healthy people, and the American Heart Association supports one whole egg daily (analysis summarizing the AHA position). One large egg has about 186 mg of cholesterol, so two eggs is roughly 372 mg, above the old ceiling but not a hard limit anymore.
Individual response. About a third of people are hyper-responders whose LDL (low-density lipoprotein) and HDL (high-density lipoprotein) cholesterol rise more with dietary cholesterol (Greene and colleagues, 2006), and APOE4 carriers may fall into that group more often, since the variant is linked to increased intestinal cholesterol absorption and greater LDL responsiveness to dietary fat and cholesterol (review of APOE and lipid metabolism), though the genotype-response findings are contested and some studies show no difference (ApoE genotype and diet study). So two eggs a day is fine for most people, but a cholesterol-responsive APOE4 carrier might see LDL move, which a follow-up lipid panel would catch. For anyone who wants the choline from eggs without raising cholesterol, the plant sources in the table cover the same ground.
The hard case. Without eggs, hitting the target gets difficult. Analyses of national intake data show that people who do not eat eggs rarely reach the recommended amount from food alone (Wallace and Fulgoni, 2017). Vegans and vegetarians are the group most likely to fall short, and a supplement or a deliberate emphasis on soybeans, cruciferous vegetables, and wheat germ helps close the gap.
A day in numbers for an APOE4 carrier. The target is the same for carriers, 425 mg a day for women and 550 for men, and among the lower-red-meat foods only soybeans are dense. Roasted soybeans carry about 107 mg per half cup, while edamame, the immature green beans, are more watery and hold less, closer to 100 mg per cup, so it takes roughly 2 cups of edamame to match a cup of roasted soybeans. Finfish and chicken sit near 70 mg per 3 oz, and other legumes near 32 mg per half cup, so soybeans do most of the work.
Without eggs, a day reaching 425 mg is 1 cup of roasted soybeans (214), 3 oz of shrimp (115), 3 oz of chicken (72), and a half cup of beans (32), about 433 mg.
With one egg, which supplies 147 mg on its own, one egg plus 1 cup of roasted soybeans (214) plus a 3 oz serving of fish or chicken (70) reaches about 431 mg.
For the 550 mg target in men, add one more dense serving, a second egg or another half to full cup of roasted soybeans.
How foragers got enough choline
The shortfall is a modern development rather than an ancestral one.
They ate the whole animal. Hunter-gatherers prized organ meats, which are the richest choline sources. Beef liver runs about 356 mg per three ounces, more than double a large egg, and brain tissue is dense in the same phospholipids that choline builds. Wild game muscle meat lands in a similar range to beef, roughly 70 to 120 mg per three ounces. Fish and shellfish are solid sources, and wild bird eggs were eaten seasonally, so a forager eating game, organ meats, and fish across a week would comfortably exceed the target.
The recent shortfall. The body also makes a little choline on its own, which covers part of the need. The roughly 90 percent modern shortfall traces to dropping organ meats, eating muscle meat without the offal, and leaning on processed foods, rather than to anything our ancestors faced.
Why your genetics change the number
PEMT and estrogen. The body makes some choline on its own through an enzyme called PEMT, and that pathway is switched on by estrogen. A common variation in the PEMT gene reduces this internal production, and the effect is stronger in women after menopause, when estrogen falls (da Costa and colleagues, 2006). Estrogen therapy lowers this requirement, with about four times fewer postmenopausal women developing liver or muscle dysfunction on a low-choline diet when given estrogen rather than placebo (Fischer and colleagues, 2010). Two people eating the same diet can therefore have different real requirements.
Folate and TMAO genes. Choline shares a job with folate, supplying small chemical tags called methyl groups that the body attaches to other molecules in many reactions, so when folate runs low the demand for choline rises. Separately, a gene called FMO3 governs how much ingested choline gets turned into TMAO, which is why the cardiovascular trade-off of high intake is partly individual. These are the kinds of factors that make a single target number imperfect.
Why choline status is hard to test
The buffered marker. A blood choline level is not a reliable readout, because the body defends it. Plasma free choline stays in a narrow band, roughly 7 to 20 micromoles per liter, and does not drop much even after more than a week without food (NIH ODS). A normal value does not confirm that intake is adequate.
The better proxies. Homocysteine and liver enzymes are more informative than a plasma choline level, though both are indirect and non-specific, and they look useful mostly because the plasma free choline they are measured against is close to useless, which is a low bar. Homocysteine mostly tracks folate and vitamin B12 status rather than choline, and liver enzymes rise only once deficiency is severe, so neither is a reliable choline readout. TMAO can be ordered through consumer labs, but that measures the downstream cardiovascular metabolite, not choline status itself.
What may be coming. A validated status test is in development, with a 2026 study using stable-isotope tracers identifying labeled betaine and phosphatidylcholine as the first circulating markers shown to separate low from adequate choline intake (2026 biomarker-panel study).
What choline supplements can and cannot do
The forms. Supplemental choline comes mainly as choline bitartrate, which is inexpensive but reaches the brain poorly and generates more TMAO, and two brain-targeted forms, citicoline and alpha-GPC (alpha-glycerylphosphorylcholine), both sold as supplements in the United States and as prescription drugs in several other countries. I graded these forms against other cognitive supplements in my review of nootropics and neurorestoratives.
The evidence in people who already have impairment. Alpha-GPC has modest randomized support for slowing decline once impairment is present. An older placebo-controlled trial in mild-to-moderate Alzheimer’s reported cognitive improvement at 1200 mg per day (De Jesus Moreno Moreno, 2003), the ASCOMALVA trial found that adding alpha-GPC to a standard Alzheimer’s drug slowed decline over two years in patients with coexisting blood-vessel damage in the brain (Amenta and colleagues, 2014), and a more recent trial in mild cognitive impairment showed a small benefit (Jeon and colleagues, 2024).
The prevention gap. Citicoline has its own Cochrane review, which found some positive effect on memory and behavior in the short to medium term in older people with cognitive impairment, though it was limited by short study duration (Fioravanti and Yanagi, 2005). That evidence, like the alpha-GPC trials, sits in people who already have impairment, not in healthy adults. A systematic review in healthy adults found no clear cognitive improvement from choline supplements (Leermakers and colleagues, 2015), and there is no completed prevention trial showing that a supplement delays the onset of dementia, so claims that pills prevent Alzheimer’s run ahead of the evidence.
The stroke signal that complicates high-dose alpha-GPC
The study. A population-based analysis of more than 12 million Korean adults aged 50 and older found that alpha-GPC users had a higher 10-year stroke risk than non-users, rising with the amount used (Lee and colleagues, 2021). The suspected reason is the same TMAO pathway, since alpha-GPC is a form of choline and a high intake can raise that gut-derived metabolite.
The counterweight. The study is observational, and alpha-GPC is prescribed to people with cognitive concerns, who may carry more baseline risk despite statistical adjustment. A later analysis in newly diagnosed mild cognitive impairment did not find the same effect. The signal is a reason for caution about long-term high-dose use in older adults rather than a settled conclusion, and it weighs more heavily than for citicoline, which does not carry the same association and was given to more than 2,000 patients in a randomized acute-stroke trial without a safety signal (Dávalos and colleagues, 2012).
Future directions
The drug pipeline. The cholinergic-agonist idea has revived after years of failures. The most advanced is xanomeline-trospium (KarXT, sold as Cobenfy and already approved for schizophrenia), a muscarinic agonist now in Phase 3 for Alzheimer’s psychosis, agitation, and cognition, with the alpha-7 nicotinic modulator MK-1167 behind it in Phase 2 (2026 pipeline review). These target the behavioral symptoms of dementia more than the underlying disease, so they sit alongside the food-and-lifestyle levers rather than replacing them.
The open question. Whether APOE4 carriers benefit from extra choline beyond adequacy will be settled by the genotype-targeted trials now underway rather than by a blood test, and a validated choline-status marker may arrive alongside them. It is also a question we are positioned to examine at NeuroAge, where we pair APOE genotype with multi-modal measures of brain aging and collect each person’s supplement use and lab values, including the liver enzymes and homocysteine that track choline status, which lets us study how choline intake relates to brain aging in carriers as our datasets grow.
What to do with this information
What to track. The useful markers are the ones that move with choline status, liver enzymes and homocysteine, rather than a plasma choline level, which the body holds steady. Individual factors like kidney function, baseline LDL, and genotype change the calculus, so this is a framework rather than a prescription.
Food first. I would not reach for a supplement as a default. For prevention in cognitively healthy people there is no completed trial showing a choline pill delays dementia. The U-shaped intake curve and the safety signals around TMAO and alpha-GPC also point against pushing past adequacy. The position with the best support is reaching the Adequate Intake from food, 425 mg a day for women and 550 mg for men, which carries essentially no TMAO or stroke concern.
For APOE4 carriers. The practical food approach leans on fish, poultry, soybeans, and other legumes, which deliver choline with little saturated fat, and fish also adds omega-3 fats. Eggs are fine in moderation with an eye on the LDL response, while red meat and liver are better kept occasional given the saturated-fat and cholesterol sensitivity that comes with the variant. As a rough anchor, 1 cup of roasted soybeans plus one egg and a 3 oz serving of fish or chicken clears the 425 mg target for women, with men adding one more dense serving to reach 550 mg.
When a supplement makes sense. Supplements earn a place mainly for people who cannot hit the target from food, chiefly vegans and vegetarians, and there citicoline is the cleaner choice than alpha-GPC on the safety side, at a common dose of 250 to 500 mg a day. Someone who wants to try a supplement could reasonably choose citicoline, keeping in mind that its positive evidence is in people who already have cognitive impairment and that nothing yet shows it prevents decline in healthy people. At the usual 250 to 500 mg dose the TMAO concern is minor, since citicoline is only about a fifth choline by weight and adds roughly 100 mg, so the rule is simply not to take large doses rather than to avoid it. The APOE4 case for extra choline is mechanistically real but rests on a 15-person Phase 1 with biomarker endpoints, so for a carrier it is a reasonable personal decision made with a clinician, food-first and with an eye on the lipid and cardiovascular response rather than reflexive high-dose pills. As an APOE4 carrier, I do not currently take a choline supplement and aim to get it from food.

Written by
Dr. Christin Glorioso, MD PhD
Dr. Glorioso is the founder and CEO of NeuroAge Therapeutics. With her background in neuroscience and medicine, she is dedicated to revolutionizing brain health and helping people maintain cognitive vitality.
Learn more about Dr. Glorioso

