
Nootropics and neurorestoratives graded by the evidence
The question I get most about brain supplements and drugs is about what works and what people should take. The first thing I want to know about a compound is which of two camps it belongs to, because that distinction shapes what to expect from it and whether the effect lasts. In practice only about a dozen of these have solid human evidence for a specific, defined use, while more than a dozen of the most heavily promoted compounds have evidence that is incomplete or unimpressive. The sensible approach as a consumer is to match an evidence-backed option to a clear goal, and to explore the less-proven ones one at a time, keeping in mind that they may not work, may not work for a given person, or may carry side effects or interactions with other medications.
The first camp is the nootropics, a term coined in the early 1970s by Dr. Corneliu Giurgea for compounds meant to improve cognition with low toxicity, and now used broadly for cognitive enhancers and smart drugs. These improve how the brain performs while the compound is present, and the benefit fades once it clears. Corrective lenses work the same way. They sharpen vision the moment you put them on, and eyesight returns to its starting point the moment you take them off. The lens never alters the eye.
The second camp is the neurorestoratives, the interventions meant to restore or preserve the structure and function of the brain in ways that hold after the intervention stops, because the underlying tissue has changed rather than its moment-to-moment operating state. This camp spans restoring what has been lost and slowing the rate at which it is lost.
This guide covers the options with the most clinical evidence in each camp, and what each is best suited to. Most of what is marketed for the brain belongs to the first camp, a smaller and more demanding set belongs to the second, and a few interventions fall between them.
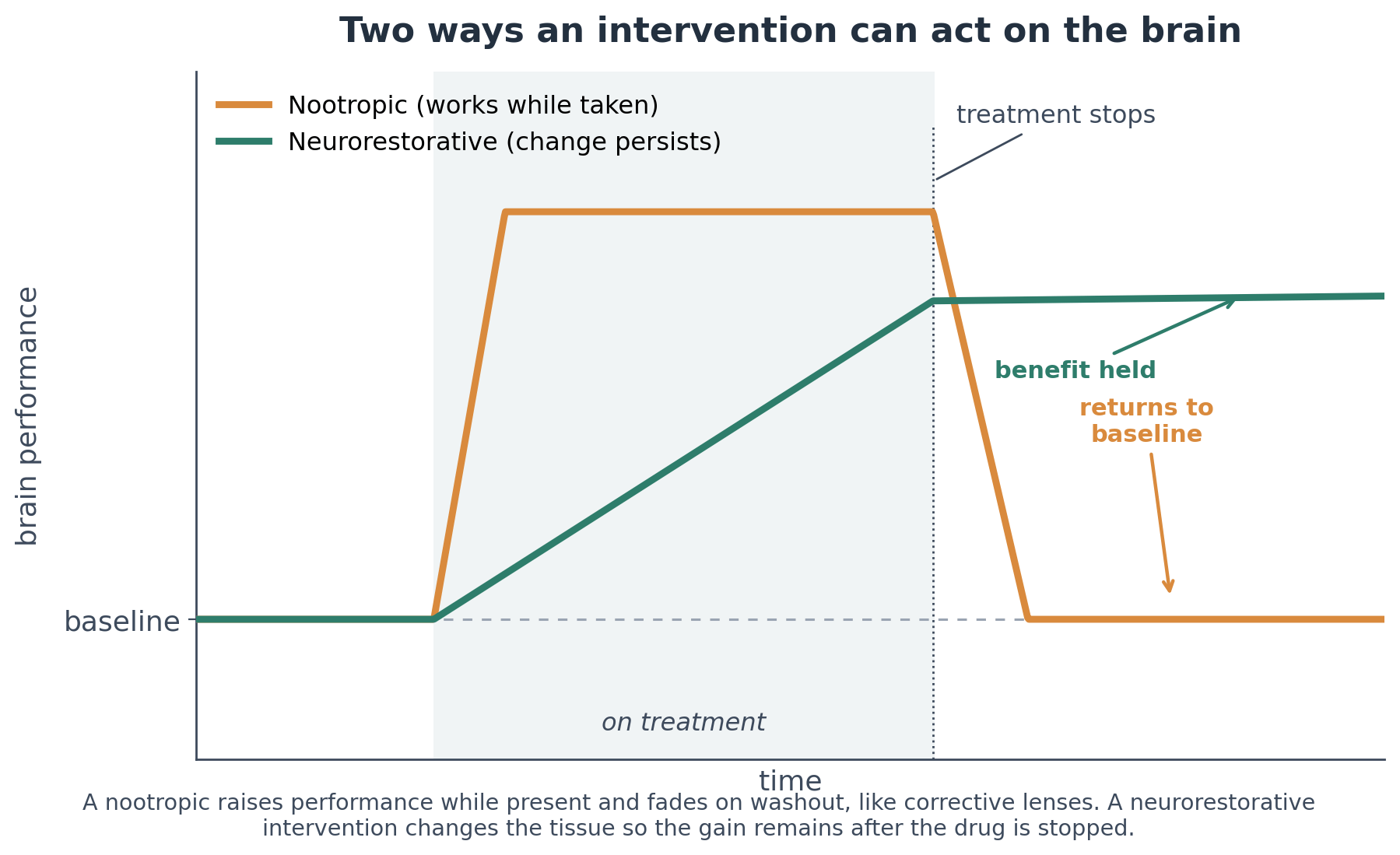
A nootropic raises performance while it is present and fades on washout. A neurorestorative changes the tissue, so the gain remains after the intervention stops.
A single question sorts any brain compound into one camp or the other
The simplest way to classify a compound is to ask what happens after you stop taking it. If the benefit disappears within days, it was tuning the function of circuits that were already intact, which makes it a nootropic. If the benefit holds, the intervention changed something durable about the tissue, its connectivity, its vasculature, or its cellular state, which makes it neurorestorative.
Mechanism separates the two camps as cleanly as the washout test does. Nootropics act on signaling, meaning the levels and balance of neurotransmitters and the excitability and gain of a network. Neurorestoratives act on the machinery and the accumulated state of the tissue, including the energy supply of neurons, the burden of damaged proteins, the level of inflammation, and the health of small blood vessels.
Brain aging shows up on three different measures
Before ranking what changes brain aging, it helps to lay out the three main ways it is measured, since these are the readouts usually assessed when determining efficacy.
The first comes from the blood, where DNA methylation clocks such as Systems Age from TruDiagnostics, Proteomics-based aging clocks like those from Vero, and RNA signatures read the activity of brain specific aging-associated genes, which is the basis of the NeuroAge panel.
The second comes from cognition, where tests of memory, processing speed, and executive function measure how the brain performs against age.
The third comes from brain MRI, where structural imaging tracks the volume of regions like the hippocampus and the thickness of the cortex and models estimate a brain-predicted age from a scan. Volume is a coarse readout, since it can rise from new synapses, small blood vessels, the birth of new neurons, which the adult brain does appear to make, or shifts in glia and fluid.
These measures generally move together, and reading across all three gives a fuller picture than any single number.
These nootropics have the strongest evidence for in-the-moment cognition
This camp has the most options on the market, and several have solid randomized evidence.
Caffeine blocks adenosine receptors to reduce the sense of fatigue and raise arousal, and it has more controlled trials behind it than any other cognitive enhancer, which makes it the reliable choice for alertness and sustained attention. Part of what regular users feel is the reversal of withdrawal rather than a gain above their true baseline, so the pure effect is smaller than the trial count suggests. Taken as coffee or tea it arrives with polyphenols, the chlorogenic acids in coffee and the catechins in tea, and both beverages are linked to lower all-cause mortality in large cohort studies, which sets the drink apart from a caffeine pill.
Caffeine with L-theanine, an amino acid from tea that shifts the brain toward a calmer and more focused state, is the better option for steady attention with less of the jitteriness of caffeine alone. A 2025 meta-analysis of randomized trials found small-to-moderate improvements in attention and task switching.
Prescription stimulants, methylphenidate and the amphetamines, raise synaptic dopamine and norepinephrine and are the first-line treatment for ADHD. In people without ADHD a meta-analysis of 48 placebo-controlled trials found only small effects on inhibitory control and memory, and its authors noted that much of what healthy users feel may be improved energy and motivation rather than faster thinking.
Modafinil, a wakefulness-promoting agent that raises cortical catecholamines and was developed for narcolepsy, has the firmest evidence among prescription options used off-label, and it suits longer and more demanding work. A 2015 systematic review found measurable gains in attention and executive function in people who are not sleep deprived, modest in size and clearest on complex tasks.
Guanfacine, an alpha-2A adrenergic agonist first used for blood pressure and now approved in an extended-release form for ADHD, strengthens prefrontal working-memory circuits. Work from Dr. Amy Arnsten’s group showed that it acts on the dendritic spines of prefrontal neurons by closing HCN ion channels, raising the gain of the networks that hold information in mind while the drug is present. Its effect is clearest in ADHD and minimal in healthy people, and because it tunes signaling rather than changing tissue, it stays a nootropic.
Creatine, a compound stored in muscle and brain that buffers the cell’s energy supply through the phosphocreatine system, is warranted for performance under metabolic stress, sleep deprivation in particular. A 2024 randomized trial found that a single high dose reduced the decline in processing speed and memory during overnight sleep deprivation, with a smaller effect in rested people. I covered the mechanism in more detail here.
Bacopa monnieri, an Ayurvedic herb whose active bacosides act on antioxidant and synaptic signaling pathways, is suited to gradual memory support rather than acute enhancement. A meta-analysis of nine trials found improvements in memory and attention, but only with daily dosing over roughly twelve weeks.
Nicotine, an agonist at nicotinic acetylcholine receptors, produces a measurable improvement in attention. Most of smoking’s cardiovascular harm comes from combustion rather than nicotine, and nicotine replacement therapy has not raised cardiovascular event rates even in people with stable coronary disease. Non-inhaled nicotine still raises heart rate and blood pressure and is not free of vascular effect, and its addiction potential is the main reason for caution. I covered the nootropic case and the delivery routes that avoid the smoke here.
L-tyrosine, citicoline, alpha-GPC, and the racetams have thinner support, though not none. A review of randomized trials found that L-tyrosine, a precursor to dopamine and norepinephrine, helped maintain attention and reaction time under acute stressors such as cold or sleep loss, with no clear benefit at rest. Citicoline and alpha-GPC are both delivery forms of choline, the nutrient cells use to make the neurotransmitter acetylcholine and the phospholipids that build membranes, and citicoline improved memory over twelve weeks in a randomized trial in older adults with age-related memory complaints. The racetams, a family of synthetic compounds built around a pyrrolidone ring, of which piracetam is the original, remain popular but have little good modern trial evidence in healthy adults.
Omega-3 fatty acids, the EPA and DHA in fish oil that form part of every neuronal membrane, are mixed to null as a cognitive enhancer in healthy adults. A large randomized trial in older adults found no effect of EPA and DHA on cognitive function, and the broader trial record shows little benefit in cognitively healthy people or in established Alzheimer’s, with a possible signal in early cognitive impairment and in people who do not carry APOE4. I covered the dietary side, where the picture is more favorable, here. Its result on aging, below, is the reason the same compound appears in both camps.
Menopausal hormone therapy is a women-specific case, included here for its effect on the cognitive symptoms of the menopause transition. Up to 70 percent of women report memory or concentration problems during perimenopause or post-menopause, with brain fog showing up as word-finding trouble, slower recall, and difficulty concentrating. It tends to be most prominent during perimenopause and usually resolves after menopause, and it is not normally a sign of permanent decline. For symptomatic women near menopause, hormone therapy can ease that fog, mostly by improving sleep and reducing hot flashes rather than through a direct cognitive effect. The longer-term picture is timing-dependent, since started near menopause it appears cognitively safe and may track with lower dementia risk, and the FDA removed the boxed warning, including the probable-dementia language, in 2026.
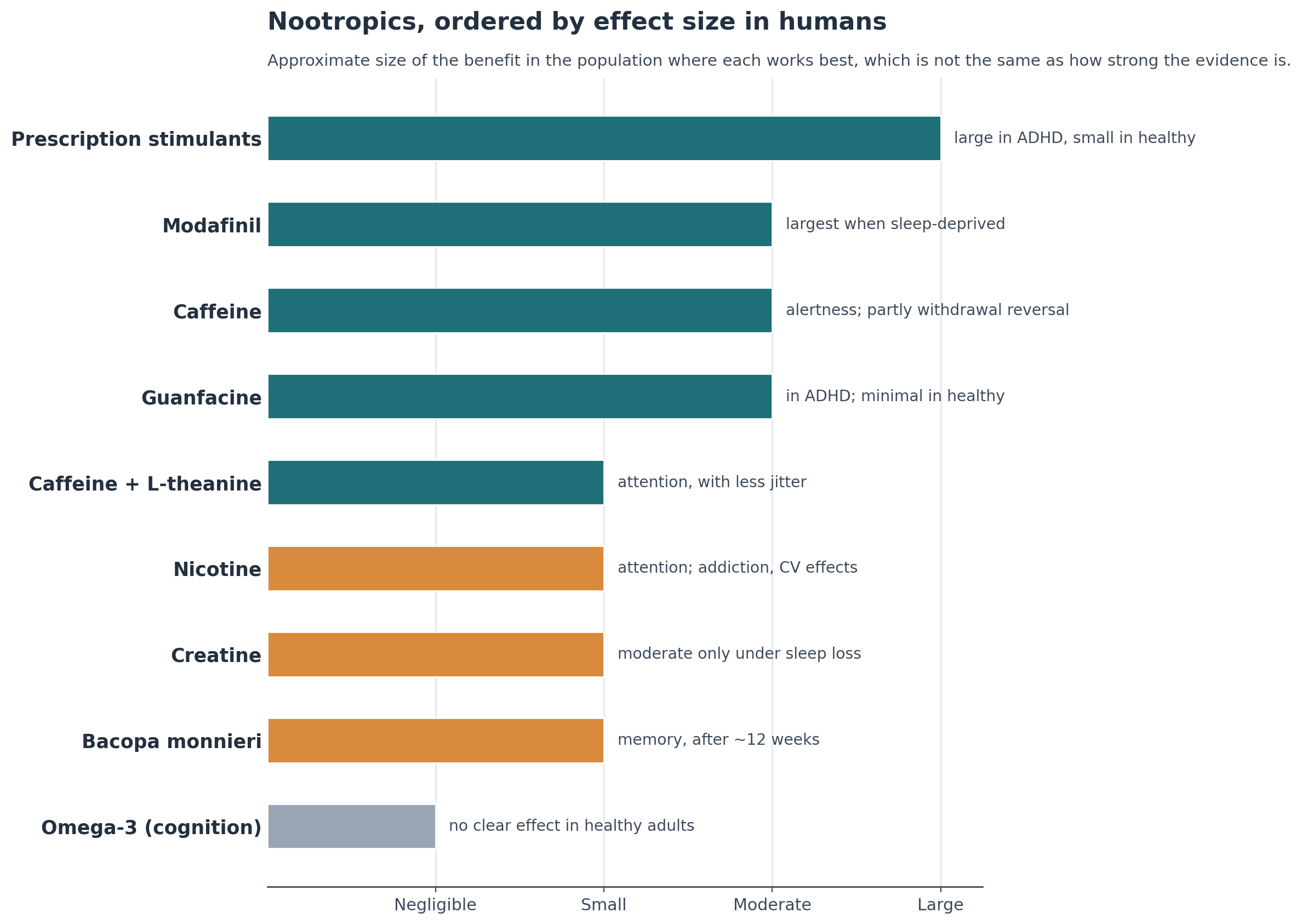
Ordered by the approximate size of the benefit in humans, which depends on the person and the task and is not the same as how strong the evidence is. Caffeine has the deepest evidence base, but prescription stimulants produce the largest cognitive effect, mostly in people with ADHD. Color reflects the current evidence, teal for a supported benefit, amber for a context-dependent benefit, gray for little or no measured effect.
What every option in this camp shares is that the benefit lasts only as long as the dosing does, and within days of stopping, performance returns to where it began.
These neurorestoratives have the most evidence for lasting change
The interventions in this camp aim at the structure and function of the brain rather than its moment-to-moment performance, and they range from restoring lost structure to slowing the rate of loss.
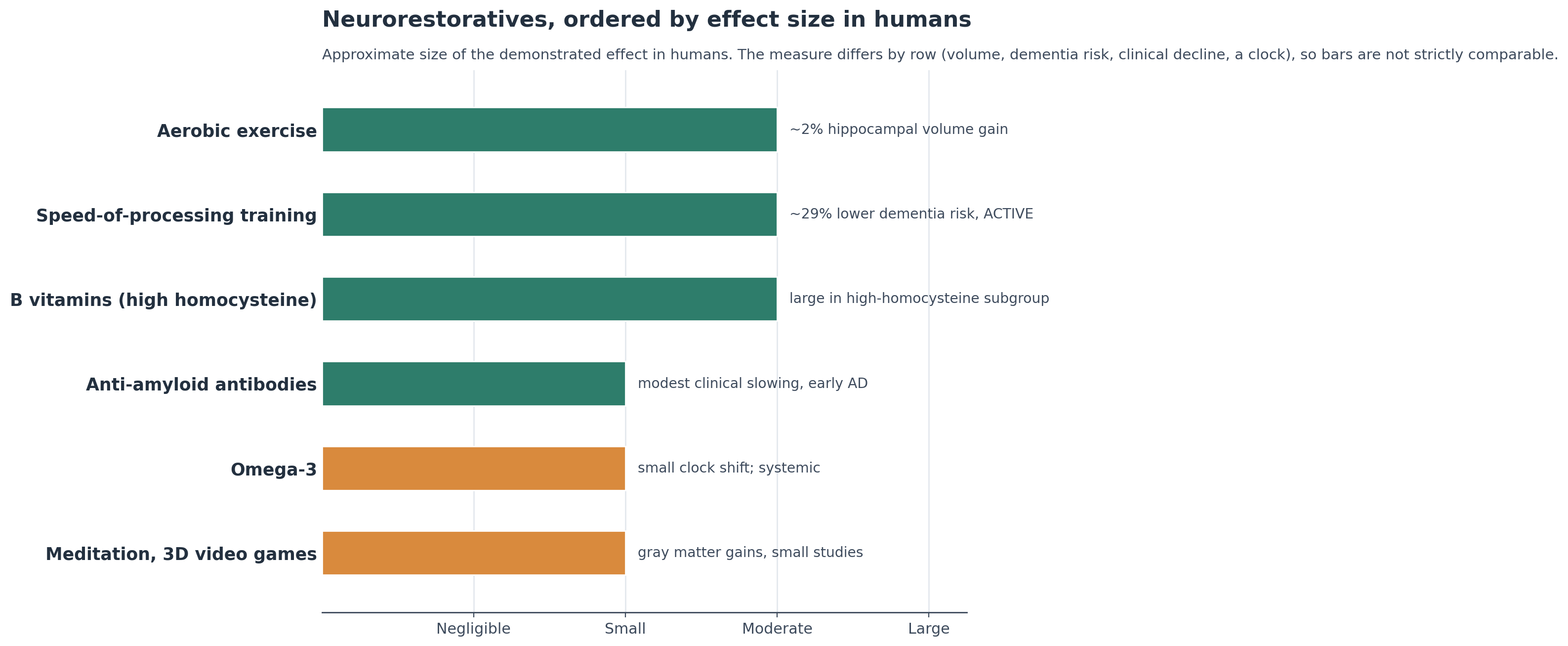
Ordered by the approximate size of the demonstrated effect in humans. The measures differ across rows, including hippocampal volume, dementia risk, clinical decline, and an aging clock, so the bars are not strictly comparable, and a larger bar reflects a larger measured effect rather than stronger evidence.
Aerobic exercise has the strongest evidence and the clearest claim to restoring a structural measure. In a one-year randomized trial in older adults, a walking program increased anterior hippocampal volume by about 2 percent, while the same region shrank by about 1.4 percent in the control group, against a normal loss of 1 to 2 percent a year at this age.
Speed-of-processing training, a computerized exercise that trains how fast the brain takes in visual information, has produced the most durable outcome of any cognitive training. In the randomized ACTIVE trial in older adults, about ten hours of it lowered the risk of dementia by roughly 29 percent over ten years, and a 20-year follow-up found that the speed arm with booster sessions was the only training type with a lasting reduction in dementia diagnoses, and NeuroAge offers a training game inspired by it. I covered the trial and why this form of training behaves differently here.
Mindfulness meditation and 3D video game training point in the same structural direction on briefer evidence. Controlled studies found gray matter increases on MRI after an eight-week mindfulness program and after two months on a 3D video game, in the hippocampus among other regions, though these were short studies of volume rather than long-term cognition.
Anti-amyloid antibodies (lecanemab, donanemab) are monoclonal antibodies that bind and clear amyloid-beta, the protein that aggregates into plaques in Alzheimer’s disease, and they are the clearest disease-modifying drugs to reach the clinic. In phase 3 trials, lecanemab and donanemab slowed clinical decline in early Alzheimer’s by roughly a quarter to a third over eighteen months, with a known risk of amyloid-related brain swelling and small bleeds. They slow the disease rather than restoring lost function, and the evidence is specific to people who already have early Alzheimer’s with confirmed amyloid, though secondary prevention trials are now testing whether clearing amyloid in cognitively normal but amyloid-positive people can delay the disease.
B vitamins, meaning folic acid with B6 and B12, lower homocysteine, an amino acid tied to vascular and neuronal damage, and they help a specific subgroup. In the VITACOG trial, high-dose B vitamins in older adults with mild cognitive impairment and elevated homocysteine reduced atrophy in the gray matter regions most vulnerable to Alzheimer’s disease, with the placebo group losing about 3.7 percent and the treatment group about 0.5 percent over two years. The treated brains still lost volume, so this slowed the loss rather than restoring tissue, and the benefit was tied to having high homocysteine to begin with.
Omega-3 acts on a different measure. In a 2025 analysis from the DO-HEALTH trial, led in part by Dr. Steve Horvath, a gram a day slowed several DNA methylation clocks of biological aging over three years, around three to four months across the clocks, with an added benefit when combined with vitamin D and exercise. The analysis was done after the fact rather than as a primary endpoint, and the clocks were measured in blood, so they track systemic aging rather than the brain in particular. It is a low-risk addition with a small effect on a molecular measure of aging.
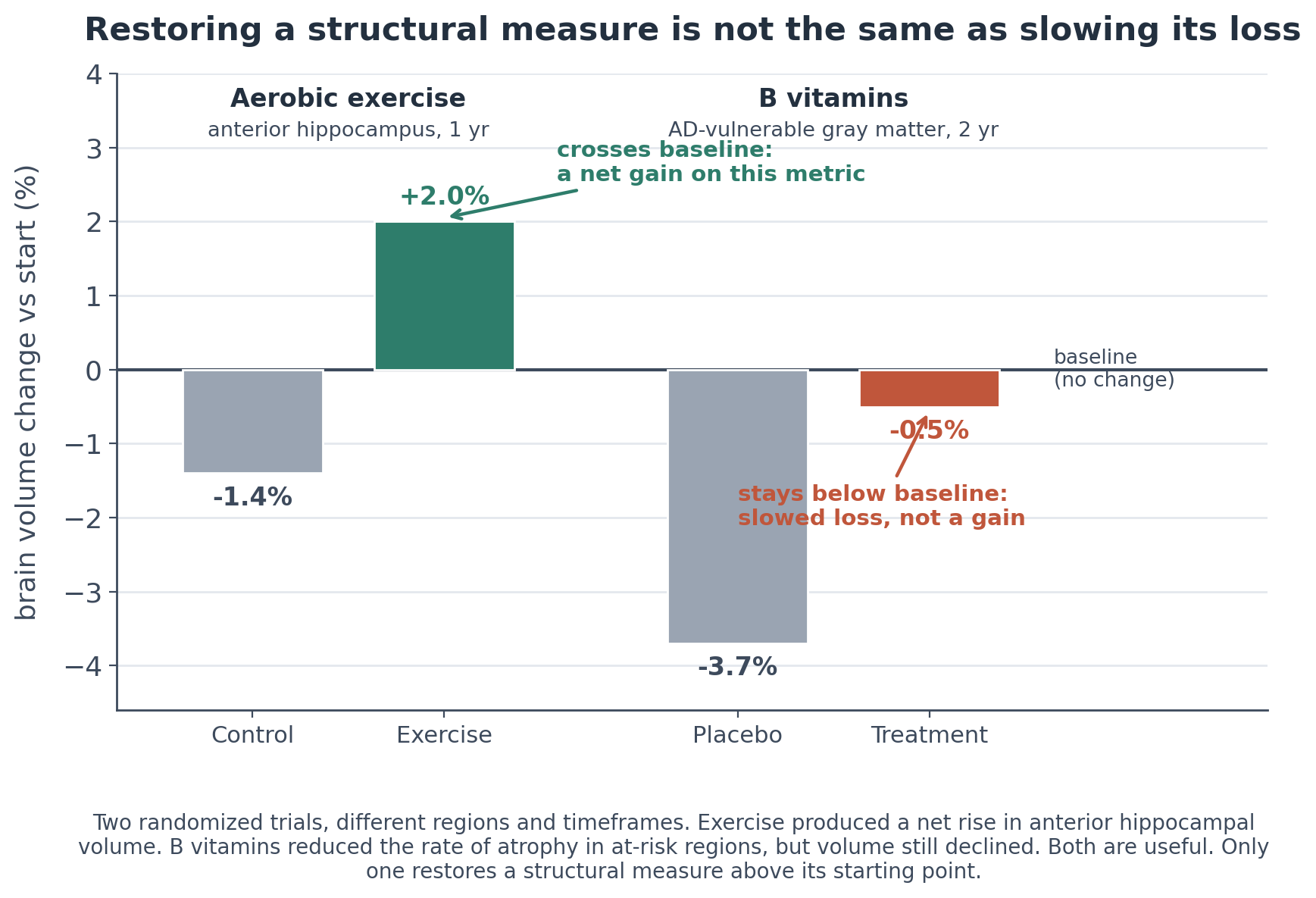
Two randomized trials, different regions and timeframes. Exercise produced a net rise in anterior hippocampal volume. B vitamins reduced the rate of atrophy in at-risk regions, but volume still declined. One restores a structural measure, the other slows its loss.
Everything else marketed for brain aging, from NAD+ precursors and senolytics to metformin, rapamycin, and CoQ10, has either failed in human trials or has not been tested in the brain at all, which is why those belong in the promotion section below rather than here.
Some interventions sit between the two camps
A few options produce effects that outlast a nootropic’s washout but fall short of a permanent structural change.
Transcranial magnetic stimulation (TMS), in which patterned magnetic pulses drive the brain’s own plasticity, induces changes that resemble long-term potentiation and outlast the stimulation period, so a course of sessions can hold its effect for a while rather than only while the device runs. Meta-analyses find it improves cognition in mild cognitive impairment and early Alzheimer’s, with one review putting the benefit at roughly four to twelve weeks per course, longer than a nootropic’s washout and shorter than a durable structural change, and it usually needs maintenance. The evidence in healthy people seeking enhancement is weaker than in impaired groups.
40 Hz gamma stimulation, which uses flickering light and sound to drive brain rhythms, rests on striking mouse work from Dr. Li-Huei Tsai’s group, where the stimulation cleared amyloid and engaged the brain’s waste-clearance system, which I reviewed here. The human results are mixed, with small open-label studies encouraging but the controlled phase 2 OVERTURE trial missing its primary endpoint, and the larger pivotal trial has finished enrolling with results pending, so for now it is best read as mechanistically promising and clinically unproven.
Ketamine and psilocybin each produce a brief acute experience but set off a wave of synaptic growth afterward, ketamine through glutamate release and mTOR-dependent synapse formation and psilocybin through rapid, lasting growth of dendritic spines in the frontal cortex, both via BDNF signaling, which is why a single session can shift symptoms for weeks. Ketamine, as the nasal spray esketamine, is approved for treatment-resistant depression, and psilocybin has shown lasting benefit after one or two sessions in depression trials. A 2025 UCSF open-label pilot in Parkinson’s disease, the first test of a psychedelic in a neurodegenerative disease, found that two sessions improved mood, cognition, and motor symptoms for weeks to months, with a larger randomized trial now under way. Whether the connections they seed harden into durable structure or fade the way a TMS course does is the same open question.
These compounds are heavily promoted but the human evidence is not in yet
More than a dozen compounds dominate the longevity and biohacking conversation. A few have real human evidence, usually outside the brain, and most have little brain evidence at all. The chart ranks the most-promoted ones by their demonstrated effect on the brain.
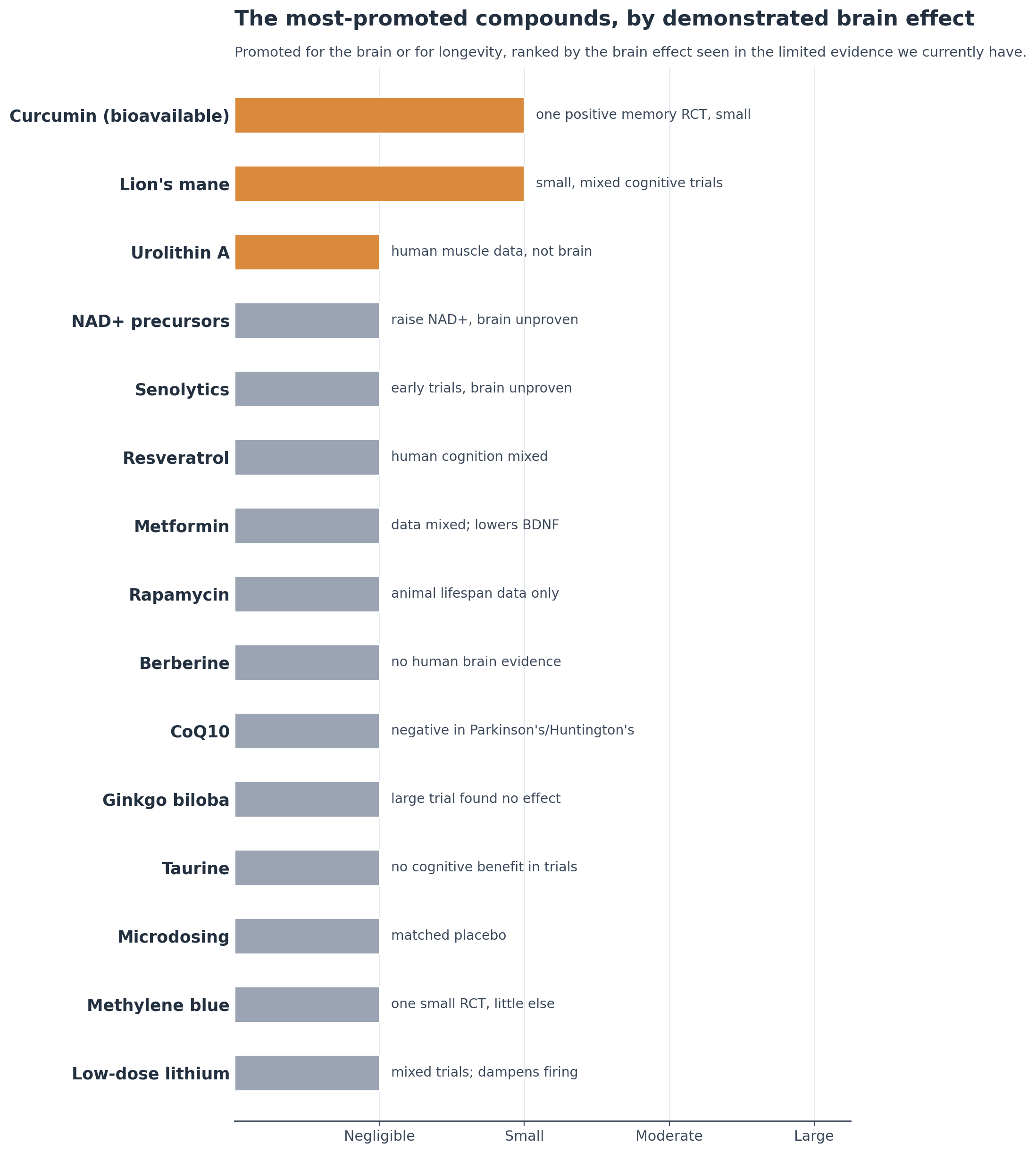
Bar length is the brain effect shown in humans, based on the limited evidence we currently have. Color reflects that evidence, amber for a real but limited or non-brain signal, gray for little, untested, or no measured effect. Most show a smaller measured effect than exercise or the prescription options.
Several are promoted mainly as longevity or anti-aging compounds.
NAD+ precursors, the vitamin B3 forms nicotinamide riboside and NMN, raise NAD+, a coenzyme for cellular energy and sirtuin activity that falls with age. They reliably increase blood NAD+, but the functional evidence for brain aging in people is mixed and emerging, and the encouraging Alzheimer’s data are still from mice. I reviewed it in detail here.
Resveratrol, a polyphenol from red grape skin once proposed to activate sirtuins, has mixed human cognition trials. A multicenter trial in Alzheimer’s disease found no benefit on cognitive or functional outcomes while shifting some biomarkers, a smaller trial in healthy older adults reported improved memory and hippocampal connectivity, and the overall assessment is that it is unlikely to help most healthy adults and that the evidence is not conclusive.
Senolytics, drugs that clear the worn-out senescent cells that accumulate with age, are the more serious candidate. The dasatinib-plus-quercetin combination cleared senescent cells in a first-in-human trial, and a small feasibility trial is testing it in Alzheimer’s, though the brain evidence is early. Quercetin and the related flavonoid fisetin occur in foods, quercetin in onions, capers, and apples and fisetin in strawberries, at amounts far below the trial doses, and whether food-level intake does anything for senescent cells has not been tested.
Metformin, the first-line type 2 diabetes drug and an AMPK activator, has cognitive data that are observational and inconsistent, and it lowers BDNF, a growth factor the brain relies on and that exercise raises, which is a reason for caution in a healthy brain. A small randomized pilot trial reported a benefit as an add-on in Parkinson’s, but the broader epidemiology is mixed and some diabetic cohorts link long-term high-dose use to higher Parkinson’s risk. I do not think it makes sense to take outside of diabetes, and I explained why here.
Rapamycin, an mTOR inhibitor used as an immunosuppressant that extends lifespan in several animals, has no brain-specific human evidence.
Berberine, a plant alkaloid that lowers blood glucose and cholesterol through AMPK and is often called nature’s metformin, has no clinical evidence for cognition or neuroprotection, only animal work.
CoQ10, a mitochondrial antioxidant, was tested at high doses in early Parkinson’s and in Huntington’s and showed no benefit, though it retains a role in blood pressure and in primary CoQ10 deficiency.
MOTS-c, a peptide encoded in mitochondrial DNA and promoted as an exercise mimetic, has metabolic effects in animals but no human brain data.
SS-31 (elamipretide), a mitochondria-targeted peptide that stabilizes cardiolipin to support energy production, became the first FDA-approved mitochondrial therapeutic in 2025, though only for the rare Barth syndrome, with the brain rationale still mechanistic and no cognitive trials. It belongs to a wider set of peptides moving through longevity and biohacker circles, including BPC-157, Cerebrolysin, Semax, Selank, Dihexa, P21, and the neurotrophic factors BDNF and klotho, whose human cognitive evidence ranges from thin to absent and which I reviewed in detail here.
GLP-1 drugs such as semaglutide, used for diabetes and obesity, are a more complicated case, because treatment failure and prevention promise point in opposite directions. The large phase 3 EVOKE trials in people who already had mild cognitive impairment or mild Alzheimer’s did not slow the disease, but the observational signal for prevention is strong, with real-world data from more than a million patients showing that semaglutide users have a 40 to 70 percent lower risk of a first Alzheimer’s diagnosis than users of other diabetes drugs. Oral semaglutide barely crosses the blood-brain barrier and the trials enrolled people relatively late in the disease, so a negative treatment result does not settle the prevention question. I reviewed the trials and the epidemiology in detail here.
Others are sold specifically for cognition.
Lion’s mane (Hericium erinaceus), an edible mushroom that raises nerve growth factor in animal studies, has human evidence that, while from small and short trials, includes real positive signals, such as faster processing on a Stroop task in healthy adults and earlier improvement in people with mild cognitive impairment. The picture is mixed and no large trial has been done, so it is promising rather than proven.
Curcumin, the polyphenol in turmeric, is held back by poor absorption, but in a bioavailable form it has the most encouraging signal here. An 18-month randomized trial in non-demented older adults found improved memory and attention and, on PET imaging, lower amyloid and tau in mood- and memory-related regions. The trial was small at 40 people and needs replication, but the result is more than marketing.
Urolithin A, a gut metabolite from pomegranate and berries sold as a mitophagy activator, has human trials showing improved muscle strength and mitochondrial markers in older adults, but the evidence is for muscle and metabolism, not the brain.
Taurine, an amino acid abundant in the body and in energy drinks, surged after a 2023 mouse study tied it to longer lifespan, but a 2025 analysis found it does not reliably decline with age in people and a meta-analysis found no cognitive benefit.
Ginkgo biloba, a plant extract long sold for memory and proposed to work through blood flow and antioxidant activity, is the clearest negative in the group. In the Ginkgo Evaluation of Memory study, more than 3,000 older adults took 120 mg twice daily for several years, and it did not lower the rate of dementia or slow cognitive decline.
Microdosing, taking sub-perceptual doses of psychedelics such as psilocybin or LSD, is promoted for focus and mood, but the largest placebo-controlled study found the benefits matched placebo. That null result is specific to sub-perceptual microdosing. Full therapeutic doses are a separate and more promising story, now in trials for depression and, as covered above, in an early test in Parkinson’s.
Methylene blue, a synthetic dye and a medication approved for methemoglobinemia that at low doses acts as an electron carrier in mitochondria, is promoted for memory on the basis of animal work and one small randomized imaging trial in 26 adults, with little other controlled human evidence. It is also a potent MAO inhibitor and carries an FDA boxed warning for serotonin syndrome when combined with SSRIs and similar drugs, a risk most clearly documented at intravenous and higher doses.
Spermidine, a polyamine found in wheat germ and aged cheese that induces autophagy, and magnesium L-threonate, a magnesium form marketed for crossing into the brain, both rest on small or preliminary trials with no clear cognitive benefit yet.
Low-dose lithium, promoted for brain aging after a 2025 Harvard study showed brain lithium is depleted early in Alzheimer’s and that lithium orotate reversed pathology in mice, has only mixed human trial evidence and works by dampening neuronal firing, so I do not recommend it for a healthy brain. I covered the trials and the mechanism here.
Some of these may be borne out as the trials read out, and the fair summary for now is that promotion has run ahead of the human evidence.
Matching the intervention to your goal is the practical step
The first step is to match the camp to the goal.
For sharper focus during a demanding stretch, caffeine with L-theanine, or modafinil where a prescription fits, with creatine useful specifically when the stretch involves sleep loss, and the benefit lasting only as long as the dosing.
For gradual memory support built over weeks, bacopa is a reasonable option.
For a lasting change in the aging brain, aerobic exercise and speed-of-processing brain training have the firmest randomized evidence, are available now, and carry minimal risk.
The rest is better guided by measurement than by default.
A homocysteine level shows whether B vitamins are likely to help.
An omega-3 index shows whether adding omega-3 makes sense.
A vitamin D level guides whether to correct a deficiency, since low vitamin D is associated with higher dementia risk in observational and genetic studies while supplementation trials for cognition have been null, so correcting a low level is reasonable and pushing it above normal is not.
APOE4 status points toward adequate choline, since Dr. Li-Huei Tsai’s group found that cells carrying the variant run their phospholipid pathway poorly and extra choline reversed the defect, a low-risk and mechanism-based option for carriers even though the targeted human trials are not yet in.
For women near menopause, menopausal hormone therapy is a reasonable option to weigh for symptoms and overall health, and it can ease perimenopausal brain fog, mostly through better sleep and fewer hot flashes.
GLP-1 drugs stand somewhat apart from this measurement-based approach. For someone who already has a reason to lose weight or lower blood sugar, a GLP-1 drug carries established metabolic and cardiovascular benefit along with the observational signal toward lower dementia risk described above, which makes it reasonable for those primary reasons. Given the long safety record of these drugs, the low microdoses some people take carry minimal risk, even if the cognition-specific trials have not been done.
For compounds that appear safe but lack the evidence, two low-risk approaches are reasonable. One is to add a single compound at a time, so any change can be attributed to it. The other is to get them from food, turmeric for curcumin, fatty fish for omega-3, berries and grapes for polyphenols, pomegranate for urolithin A, and the lion’s mane mushroom itself, foods that are healthful on their own and carry no meaningful risk.
Knowing which metric moved, and whether it rose above baseline or only fell more slowly, is what separates a lasting result from a temporary one, which is also why measuring brain aging across several markers at once gives a steadier read than any single number.
Much of the evidence that is still missing may arrive sooner than the traditional model would suggest, as AI accelerates large decentralized real-world trials that can collect human data on these interventions at a scale and pace conventional trials could not reach.

Written by
Dr. Christin Glorioso, MD PhD
Dr. Glorioso is the founder and CEO of NeuroAge Therapeutics. With her background in neuroscience and medicine, she is dedicated to revolutionizing brain health and helping people maintain cognitive vitality.
Learn more about Dr. Glorioso

