
Does speaking a second language protect the aging brain? (new study)
A new study out this month in the Proceedings of the National Academy of Sciences revived a question I get asked all the time. Does a lifetime of using more than one language protect cognition or lower the risk of dementia? The intuition behind it is easy to follow. Speaking two languages means the brain is constantly choosing one and holding the other back, a small act of mental control repeated across a lifetime, and that looks like the kind of sustained exercise that ought to build cognitive reserve. The new study adds to a now-substantial body of work, and it is a useful way into what that evidence supports and where it falls short.
The new data come from 312 adults aged 18 to 80. In the June 2026 PNAS article, researchers set out to do two things. First, they wanted to map the relationship between bilingual experience and executive function across the entire adult lifespan, using a continuous measure of bilingualism rather than the usual blunt split into “bilingual” and “monolingual.” Second, they asked whether bilingual experience might buffer the cognitive decline that some older adults reported after COVID-19, the lingering “brain fog” that has been hard to pin down. They found a coherent pattern linking two specific features of bilingual experience, an earlier age of learning the second language and higher proficiency in it, to stronger executive function across several tasks. Among the older adults, the relationship between having had COVID-19 and slower task-switching depended on when the person had learned their second language. Those who learned it later in life showed larger COVID-related differences in switching performance, while those who learned it early showed almost none. The authors frame this as moderation-based evidence consistent with cognitive-reserve models of aging, and they are careful not to claim that bilingualism prevented anything.
The choice to study a virus is less of a detour than it looks. The brain fog that follows COVID-19 falls largely in the domain of executive function, the same abilities that erode in aging, and the infection leaves a physical mark, with one UK Biobank analysis finding more gray matter loss and a larger reduction in brain size in people scanned after infection than before (Douaud and colleagues, 2022). A sudden insult like that is a natural test of resilience. If some feature of a person’s history blunts its cognitive cost, it is reasonable to ask whether the same feature blunts the slow insults of aging, which is why a study of recovery from a virus is also a study of cognitive reserve.
That phrase, cognitive reserve, carries more than one meaning, and it helps to be clear about each before weighing whether bilingualism provides any benefit at all.
How could a second language change the brain?
Researchers tend to separate three related ideas, and they make different predictions. Cognitive reserve describes a brain that copes with damage by using its networks more efficiently or flexibly, so thinking holds up even as pathology builds. Brain reserve is more physical, the amount of tissue and connection a person starts with, since more substrate means more to lose before deficits appear. Brain maintenance is the most demanding claim, that an experience actually slows the loss of structure over time rather than padding the starting amount. Bilingualism has been proposed as a route to all three, and the evidence now speaks to more than one.
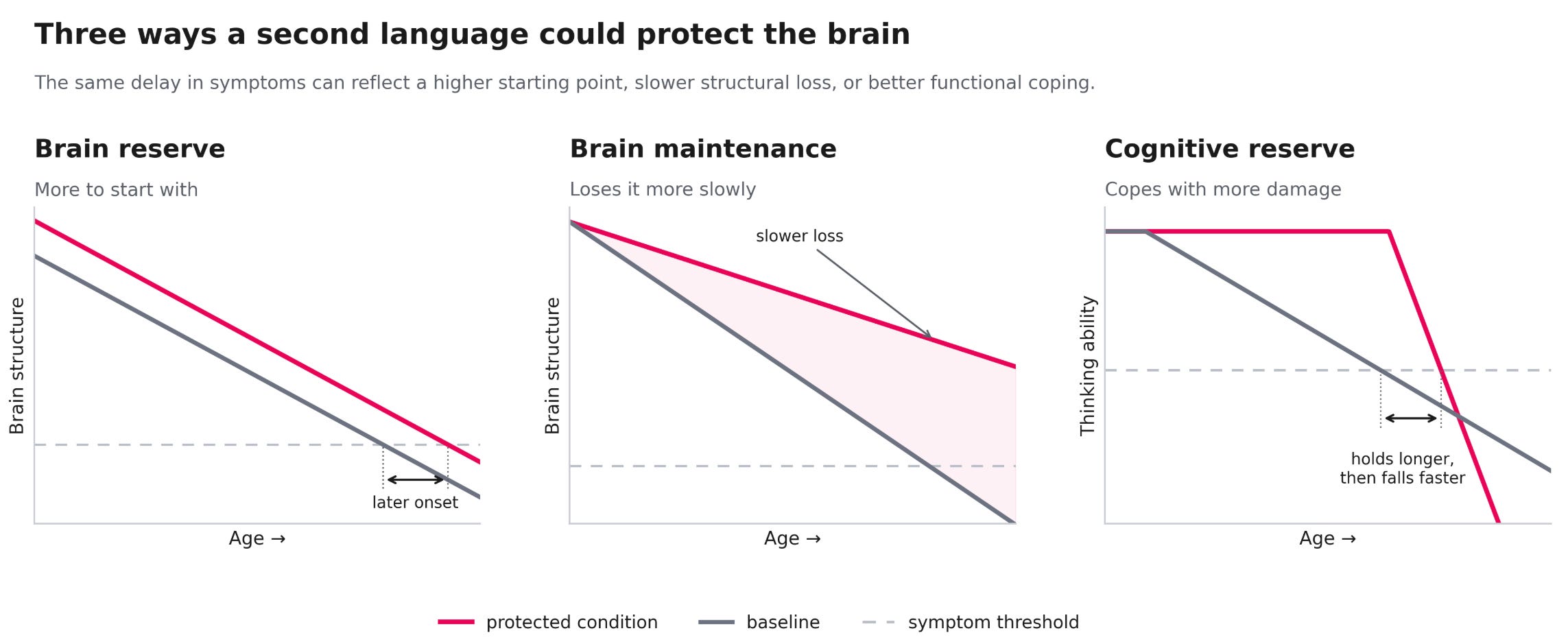
The functional case is the oldest. Bilingualism is thought to exercise frontal and executive-control networks each time the brain selects one language and suppresses the other, a low-grade workout repeated across a lifespan. The clearest fingerprint of that functional buffer comes from disease. In people who already have Alzheimer’s, bilinguals tend to show more advanced brain atrophy than monolinguals at the same level of clinical symptoms (Perani and Abutalebi, 2015). Read correctly, that supports the reserve model rather than undercutting it, because tolerating more underlying damage before symptoms appear is exactly what a functional buffer would do.
The structural case has grown alongside it. Bilingualism is associated with greater gray and white matter and thicker cortex in language and control regions, and in one comparison of older adults the monolinguals showed the expected age-related thinning of the temporal pole while the bilinguals did not (a 2015 volumetric MRI study). More education tracks with larger regional cortical volume in cognitively healthy people (a 2012 structural MRI analysis), and a large study that followed people over time found higher cognitive ability linked to slower atrophy in select regions, the signature of a brain holding onto its structure rather than simply starting with more of it (a longitudinal imaging study). These point past pure compensation toward the brain reserve and brain maintenance ideas.
The strongest causal evidence comes from watching the brain before and after learning. When adults take up intensive language study the brain responds, and a controlled before-and-after study of military interpreters found growth in hippocampal volume and in the thickness of language-related cortex over three months relative to controls (Mårtensson and colleagues, 2012). Because the change followed the training rather than preceding it, it is hard to dismiss as a pre-existing difference, although gains like these tend to be regional and can recede once the practice stops. This before-and-after design is also the cleanest answer to the objection that bilinguals differ from the start, since the brain changed after the teaching rather than the teaching following an already different brain.
These mechanisms are not mutually exclusive. A second language could build a functional buffer, add structural substrate, and help preserve that structure over time, and the evidence now points to contributions on both the functional and structural sides. The PNAS COVID result is that buffer caught mid-action, with the infection’s effect on task-switching softened most in the deepest and earliest bilinguals, reserve working as a moderator rather than a shield. What no trial has shown is the long view, that lifelong bilingualism preserves brain structure across decades, and some of the structural difference seen in older bilinguals was likely present from the start. Holding all three mechanisms in mind changes how the rest of the evidence reads. Two questions run through it, whether the protection is real and whether it comes from the language itself or from the kind of person who becomes bilingual, since bilinguals tend to be more educated and may have had higher cognitive ability to begin with, both of which lower dementia risk on their own. The study designs answer the second unevenly, so each should be read with that objection in mind, beginning with the finding that put bilingualism on the map.
A delay in symptoms is not the same as a lower risk
The foundational observation came from Dr. Ellen Bialystok and colleagues in 2007. Reviewing the records of patients seen at a memory clinic in Toronto, they reported that lifelong bilinguals showed their first dementia symptoms about four years later than monolinguals, despite similar levels of education and cognitive status at diagnosis (Bialystok, Craik, and Freedman, 2007). A reasonable objection followed almost immediately. The Toronto bilinguals were largely immigrants, and immigration carries its own basket of confounders, so perhaps something other than language was responsible. As a backward look at people who already had dementia, it is also the design most exposed to the worry that the two groups differed before any language entered the picture.
A 2013 study in a non-immigrant population addressed that objection directly. Dr. Suvarna Alladi and colleagues examined 648 patients with dementia in Hyderabad, India, a city where speaking two or more languages is an ordinary feature of daily life rather than a marker of migration. Bilingual patients developed dementia about 4.5 years later than monolingual patients, and the association held after accounting for education, occupation, sex, urban versus rural residence, and immigration status (Alladi et al., 2013). The convergence of the Toronto and Hyderabad figures, roughly four to five years in two very different settings, is a large part of why the delayed-onset finding has held up. Because that population removes the immigration objection and much of the education one at the same time, it answers two of the obvious confounds in a single setting.
A delay is what all three mechanisms would predict, so the finding alone cannot say whether the brain is masking accumulated damage or carrying less of it. What the delay does not establish is the separate claim often attached to it, that bilinguals are less likely to develop dementia in the first place. A later age of symptom onset and a lower lifetime chance of the disease are different outcomes that require different study designs, and they do not have to move together. When researchers stopped conflating the two, the picture sharpened.
The prospective evidence for lower risk is weak
The cleanest way to test whether bilingualism lowers dementia risk is to follow initially healthy people forward in time and count who develops dementia, rather than studying people who already have it and asking when their symptoms began. When the prospective studies were pooled, the protective signal mostly disappeared.
A 2017 systematic review and meta-analysis found essentially no effect on incidence. Combining prospective studies covering more than 5,500 bilingual participants, the pooled odds ratio for developing dementia was 0.96, with a confidence interval running from 0.74 to 1.23 (Mukadam, Sommerlad, and Livingston, 2017). An odds ratio that straddles 1.0 that closely is the statistical signature of no reliable association. Following healthy people forward also strips out much of the selection problem that clouds the clinic studies, since the groups are set before anyone develops dementia. The same review noted that the retrospective studies, the ones looking backward at age of onset, continued to show the delay.
A 2020 meta-analysis quantified the gap between the two questions. Pooling both retrospective and prospective work, the protective effect on age of symptom onset reached a moderate effect size (Cohen’s d of about 0.32), while the effect on whether dementia occurred at all was much weaker (d of about 0.10) (Anderson, Hawrylewicz, and Grundy, 2020). A separate systematic review the same year reached the same structural conclusion, summarizing it in its title: bilingualism is associated with a delayed onset of dementia but not with a lower risk of developing it (Brini et al., 2020).
There are exceptions that point the other way. A door-to-door community study of more than 1,200 older adults in Bengaluru, India, reported lower dementia prevalence among bilinguals than monolinguals, 0.4 percent versus 4.9 percent (reported in a 2024 community-based analysis). Prevalence studies cannot separate later onset from a lower rate of new cases, so this is consistent with the delay model rather than evidence against it, but it is a reminder that highly multilingual populations with constant language switching may behave differently from the Western samples that dominate the literature.
A delay would be far from trivial, even with lifetime risk unchanged. Because the chance of dementia climbs steeply with age and people face competing causes of mortality, pushing onset back by even a year or two means many are lost to other causes first and never reach the diagnosis. One projection estimated that delaying onset across the population by a single year would eventually leave roughly 800,000 fewer Americans with the disease, and a two-year delay close to two million fewer (Brookmeyer, Gray, and Kawas, 1998). A delay is also what a slowing or better-maintained brain would produce, so the onset finding is consistent with real protection rather than evidence against it. The open question is not whether a delay would be worth having but whether this one is real and caused by language. A sizable real delay should have pulled the prospective numbers down too, since pushing events later leaves fewer of them inside any follow-up window, so the flat incidence is part of what makes the retrospective delay look potentially confounded.
Whether the delay is about language at all is the deepest objection, and the designs answer it unevenly. Bilinguals tend to be more educated and may have had higher cognitive ability to begin with, so the effect could be one of those traits in disguise. Hyderabad already removed the education and immigration versions, holding up where many people had little schooling. The intelligence version is harder, because a more cognitively able child may simply be more likely to take up and keep a language, and ruling it out needs intelligence measured before the language. The Lothian Birth Cohort 1936 is the one design that managed it, with general intelligence scored at age 11 in 1947 for 853 people retested in their seventies, where the bilinguals exceeded the prediction from their own childhood baseline, including those who learned the language as adults and after adjusting for early intelligence, social class, and sex (Bak, Nissan, Allerhand, and Deary, 2014). What no design fully separates is bilingualism from the bundle it travels in, since education shows the same signature, a later onset followed by faster decline once symptoms begin (Meng and D’Arcy, 2012), which is what you would expect if schooling, occupation, and language are overlapping deposits into one account, the brain’s reserve, rather than separate routes to protection.
The everyday cognitive advantage is contested
Underneath the dementia question sits a broader and noisier claim, that bilinguals enjoy a general advantage in executive function, the family of skills covering attention, inhibition of distractions, and switching between tasks. This is the proposed engine behind any functional benefit, so its reliability matters.
Part of the apparent advantage may be an artifact of what gets published. Dr. Angela de Bruin and colleagues tracked 104 conference abstracts on bilingualism and executive control presented between 1999 and 2012, then checked which were later published in journals. Studies that fully supported a bilingual advantage were the most likely to be published, studies with mixed results less so, and studies that challenged the advantage the least likely of all (de Bruin, Treccani, and Della Sala, 2015). When null results sit in file drawers, the published record drifts toward a stronger and cleaner effect than the full evidence supports. This does not prove the advantage is absent, and other researchers have argued the publication-bias estimate itself was inflated by how studies were classified, but it does mean the executive-function story should be held loosely.
What seems to survive the scrutiny is narrower than the popular version. The benefits, where they appear, cluster around attentional control and task-switching rather than broad intelligence, they are larger when second-language proficiency and use are high and sustained, and they show up more consistently in brain-imaging measures of structure and connectivity than in behavioral test scores. The PNAS article fits squarely here, since its strongest signal was for task-switching specifically, and it scaled with proficiency and early acquisition rather than with the mere fact of speaking two languages.
Can you start as an adult and still benefit?
Most of the evidence above describes people who became bilingual in childhood and stayed that way. The practical question for most readers is different. If you grew up monolingual, does taking up a language in midlife or later do anything for your brain?
The cognitive intervention studies are small, short, and mixed. A one-week intensive Gaelic course improved attention switching in 33 adult learners aged 18 to 78, a gain absent in matched controls and, nine months later, maintained in those who kept practicing several hours a week (Bak and colleagues, 2016). A separate randomized trial pointed the other way, assigning 34 monolingual adults aged 65 to 80 to a three-week intensive Spanish course or a waiting list, where the effect on the primary attention measure was not significant, though learners with lower baseline cognition showed some improvement in response inhibition (results from a randomized controlled superiority trial, 2023). The broader set of trials fits that split, with brief high-intensity courses sometimes moving attention while longer or lower-intensity ones often show nothing, and the authors of the Spanish trial protocol were frank that the prior evidence was sparse and contradictory. A course measured in weeks is a thin intervention against which to detect durable cognitive change, and longer, better-powered trials are needed before anyone can say that adult language learning measurably moves cognition.
The structural side is more encouraging, and the two need not agree. The interpreter study described earlier found measurable brain growth from intensive adult study even where short cognitive trials disagree, fitting the idea that engaging, demanding learning shapes the brain whether or not a brief test battery captures it. That combination of features is the kind the reserve literature associates with healthier brain aging, a pattern that also shows up for structured cognitive training.
Why cognition is a lagging indicator of brain health
Reserve, whether functional or structural, has a consequence that reaches well beyond bilingualism. Because it lets the brain keep performing while damage builds, two people carrying the same amount of amyloid or the same loss of brain volume can score differently on a thinking test, which is why these protective experiences show their clearest effect on when decline becomes visible.
The consequence is that thinking ability is a lagging indicator. A person with substantial reserve can compensate for years, sometimes decades, while pathology accumulates quietly, and their performance on cognitive tasks stays in the normal range until the damage finally outpaces the buffer. By the time scores fall, the disease process has usually been underway for a long time. Cognition signals when reserve has been spent, not when the decline began.
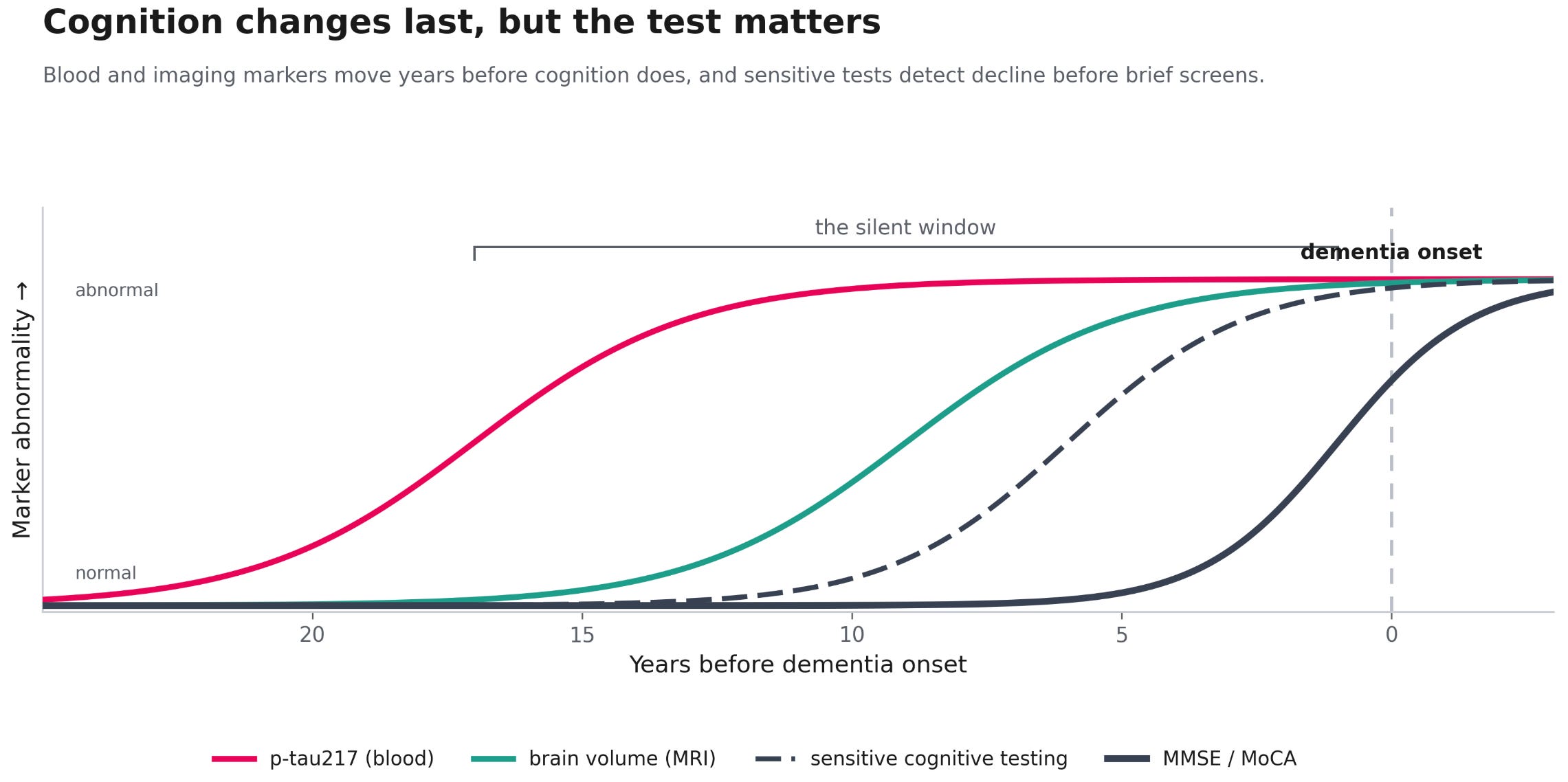
This is also why the usual cognitive screens miss early disease. The Mini-Mental State Examination and the Montreal Cognitive Assessment, the two brief tests most often used in clinics, were designed to detect impairment once it is present, not to find pathology while a person still functions normally. Someone with high reserve can score at the top of either test while carrying measurable amyloid, tau, or a reduction in brain volume (Meng and D’Arcy, 2012). The limitation is specific to brief screens. More sensitive cognitive measures, the kind developed to detect the subtle changes of preclinical disease, register decline in processing speed and memory earlier than a screen does, and a composite built for that purpose becomes less sensitive when the MMSE is folded into it (Stricker and colleagues, 2023). A normal screen is reassuring about current function, but it does not rule out a process that may already be years along, which is the window in which prevention has the most room to work.
Catching that window calls for signals that move before cognition does. Molecular and structural markers change well ahead of symptoms, with blood markers such as p-tau217 shifting more than two decades before cognitive scores register anything. This is the reason NeuroAge is built around reading the underlying biology rather than relying on test performance alone, combining RNA-based markers of the brain’s molecular aging state, brain imaging, and sensitive cognitive testing so that a person can be placed on a trajectory while there is still time to change it. No single marker captures the whole picture, but together they describe where someone sits long before a cognitive test would notice.
The bottom line
The evidence for bilingualism and the aging brain is real, but it is narrower and more conditional than the popular framing suggests. Its delayed-onset finding replicates, a delay of roughly four to five years in when dementia symptoms appear, but the prospective incidence is null and the everyday executive-function advantage is shadowed by publication bias. And the question most people care about, whether starting a language as an adult helps, has only a handful of small trials behind it with mixed results.
Set against education and exercise, bilingualism is the least certain of these reserve contributors. Because it overlaps so heavily with education, intelligence, and social class, its independent contribution on top of those is probably modest, and the flat prospective incidence is what you would expect if the incremental effect on the hard endpoint is small. The Lothian childhood-IQ data suggest some independent increment, but a small one. Weaker evidence is not the same as a smaller true effect, though. Bilingualism is hard to measure, a continuous and many-sided thing compressed into proficiency scores or a yes-or-no label, and it cannot be assigned at birth and followed for sixty years, so some of its evidentiary weakness is measurement noise and untestability rather than biological smallness.
The mechanism is where the field has moved most. Reserve buys time rather than immunity, the same way education, cognitively demanding work, and physical fitness do, a connection I have drawn before in writing about VO2 max and dementia. What the imaging and the training studies add is that the buffer is not only a matter of coping, since at least some of what bilingualism contributes looks like active change in the brain rather than a more efficient use of what was already there. That structural claim still has limits, because no trial has followed bilingualism across decades and the gains from shorter studies can recede. A second language belongs among the experiences that plausibly build and protect the aging brain rather than only mask its decline. The PNAS study is a reminder that this protection may matter not only against the slow erosion of Alzheimer’s but during sudden insults like COVID-19, where the earliest and most proficient bilinguals showed the smallest cognitive cost.
Should you fire up Duolingo to protect your brain health? I would say for sure if it’s something that you enjoy doing but it may not be much better than other forms of mental activity like taking a class, learning to play an instrument, or gaining a new hobby.

Written by
Dr. Christin Glorioso, MD PhD
Dr. Glorioso is the founder and CEO of NeuroAge Therapeutics. With her background in neuroscience and medicine, she is dedicated to revolutionizing brain health and helping people maintain cognitive vitality.
Learn more about Dr. Glorioso

