
The PCSK9 longevity gene- therapeutics, heart health, brain health, and supplements
The story of PCSK9 (proprotein convertase subtilisin/kexin type 9) is one of the most remarkable examples of translational medicine in the 21st century. In just over two decades, this protein went from an unknown player in cholesterol metabolism to the target of multiple FDA-approved drugs that are having a large impact on cardiovascular medicine. But the PCSK9 story extends beyond cholesterol—it intersects with human longevity, brain health, and the future of precision medicine.

What is PCSK9 and Why Does It Matter?
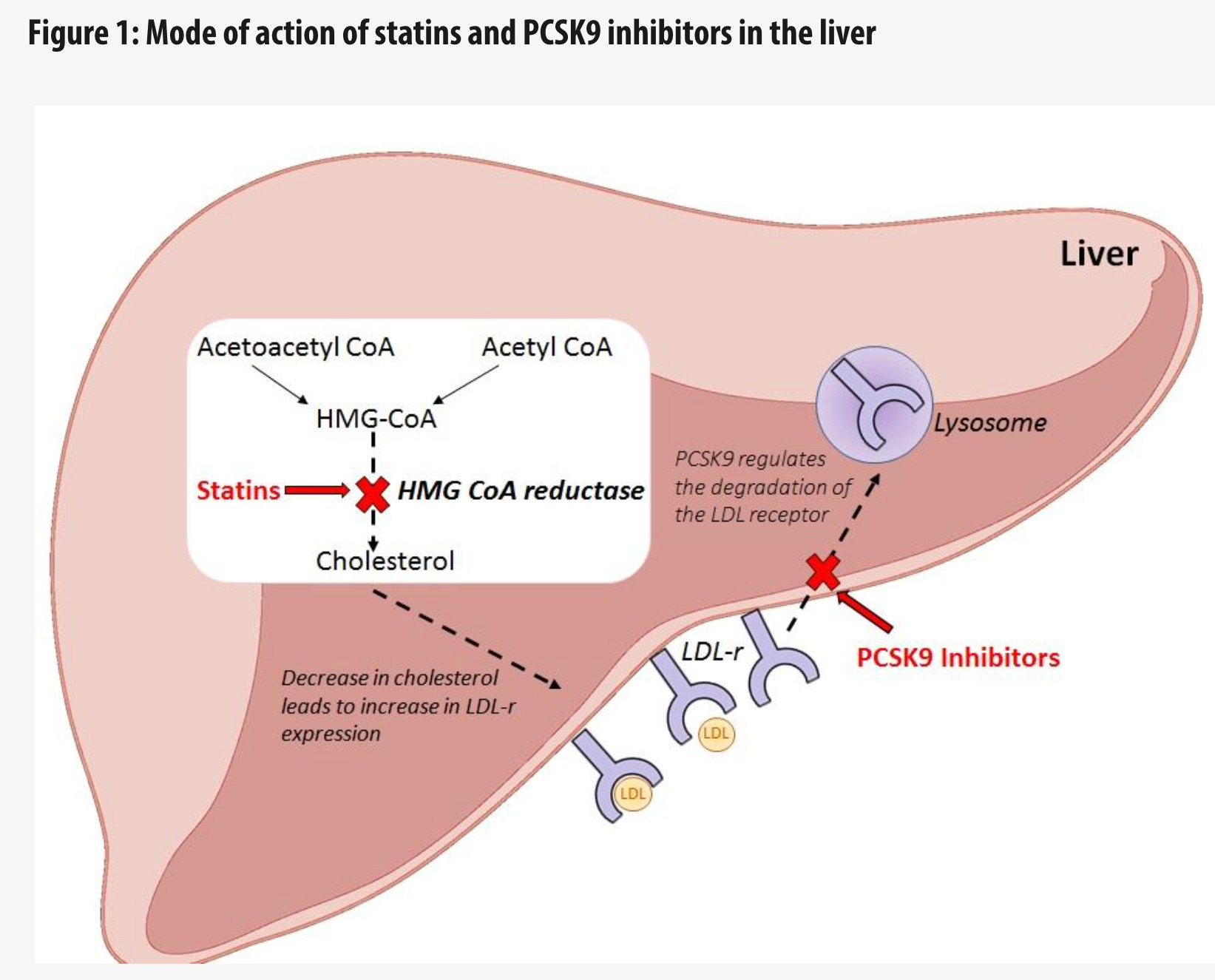
PCSK9 is a protein primarily produced in your liver that plays a crucial role in regulating LDL cholesterol levels—the so-called “bad cholesterol.” Here’s how it works: your liver cells have LDL receptors on their surface that bind to LDL cholesterol particles from your bloodstream and pull them inside for processing. PCSK9 binds to these receptors and marks them for destruction, reducing the number of receptors available to clear cholesterol. More PCSK9 means fewer receptors, which means higher circulating LDL cholesterol.
The discovery of PCSK9’s role began in 2003 when researchers identified gain-of-function mutations in the PCSK9 gene in French families with familial hypercholesterolemia, a condition that causes dangerously high cholesterol from birth. Shortly after, scientists discovered the flip side: people with loss-of-function mutations in PCSK9 had remarkably low LDL cholesterol and dramatically reduced cardiovascular disease risk.
In one landmark 2006 study, participants with these protective mutations had 28% lower LDL cholesterol and an 88% reduction in cardiovascular disease risk.
This genetic evidence was so compelling that it launched a pharmaceutical race to inhibit PCSK9- and remarkably, the first drugs were approved just 12 years after the initial discovery.
PCSK9 Inhibitors prevent PCSK9 from doing it’s job, which in turn increases the number of receptors available to clear cholesterol, lowering LDL levels. Statins work through different mechanisms by inhibiting HMG CoA reductase as well as other effects. Together the two classes of drugs are synergistic when used in combination.
PCSK9 Genetic Variants: rs505151 and rs11591147
Two PCSK9 genetic variants have emerged as particularly important for understanding individual cardiovascular risk:
rs505151: The Risk Variant (Gain-of-Function)
The G allele of rs505151 is a gain-of-function variant that increases PCSK9 activity and causes Familial Hypercholesterolemia. People carrying this variant have:
Very high triglyceride and LDL cholesterol levels
Approximately 50% increased cardiovascular risk
More aggressive LDL receptor degradation
This variant may identify people who could benefit from earlier or more aggressive lipid-lowering interventions.
rs11591147: The Protective Variant (Loss-of-Function)
The T allele of rs11591147 is a loss-of-function variant that reduces PCSK9 activity. Carriers benefit from:
10-16% lower LDL cholesterol levels throughout life
23-28% lower risk of coronary heart disease
Reduced risk of ischemic stroke
No apparent negative health effects despite lifelong low cholesterol
This variant essentially mimics what PCSK9 inhibitor drugs do—and the fact that people born with this variant live long, healthy lives with no cognitive impairment provides safety evidence for PCSK9 inhibitor therapies.
Curious whether you have these PCSK9 variants? If you’ve had your NeuroAge genetic resilience analyzed, you can check your PCSK9 genetics on your dashboard. Understanding your genetic profile can inform discussions with your healthcare provider about personalized lipid management strategies.
PCSK9, Longevity, and Lifespan
The connection between PCSK9 genetics and longevity is becoming increasingly clear through multiple lines of evidence:
Human Genetic Studies
Mendelian randomization studies- which use AI and genetic variants as natural experiments—have revealed compelling longevity effects:
Each standard deviation increase in genetically determined LDL cholesterol is associated with 1.2 years shorter lifespan
Genetic variants mimicking PCSK9 inhibition are associated with extended lifespan, particularly in men (approximately 2.4 years per standard deviation of LDL-C reduction)
The effect appears dose-dependent: more LDL lowering equals greater lifespan extension
Genetically low LDL cholesterol due to PCSK9 variants reduces cardiovascular mortality but also contributes to overall longevity
Polygenic Risk Scores
Individual PCSK9 variants have modest effects, but when incorporated into polygenic risk scores (PRS) that combine information from hundreds of genetic variants, they become powerful predictors:
People in the top percentiles of polygenic risk scores for coronary artery disease have cardiovascular risk equivalent to or exceeding monogenic familial hypercholesterolemia
These high-risk individuals derive the greatest benefit from PCSK9 inhibitor therapy—with some studies showing 37% relative risk reduction in major cardiovascular events compared to only 13% in lower-risk individuals
The implication? Genetic information can help identify who will benefit most from PCSK9 inhibitor therapy, making these expensive drugs more cost-effective by targeting those at highest risk.
PCSK9, Lipids, and Brain Health: A Complex Relationship
This is where the story gets particularly interesting—and relevant to brain aging and cognitive health.
The Brain and Cholesterol
The brain contains approximately 20% of your body’s total cholesterol, making it the most cholesterol-rich organ. Cholesterol is absolutely essential for brain function:
Myelin sheaths (the insulation around neurons) are 70% lipid by weight, with cholesterol being a major component
Cholesterol is critical for synapse formation and neurotransmitter release
Proper cholesterol metabolism is essential for memory and learning
However—and this is crucial—brain cholesterol operates almost completely independently from blood cholesterol. The blood-brain barrier efficiently prevents exchange between circulating lipoprotein cholesterol and brain cholesterol. Almost all brain cholesterol is synthesized locally within the brain itself.
What About PCSK9 Inhibitors and Brain Health?
Given that PCSK9 inhibitors can lower LDL cholesterol to levels around 25-30 mg/dL (far below normal), an obvious concern arose: could this harm the brain? The answer, based on extensive research, appears to be no:
Clinical trial evidence:
The EBBINGHAUS trial followed 1,204 patients on evolocumab for 1.6 years with detailed cognitive testing and found no adverse effects on cognitive function
Multiple other trials have confirmed the cognitive safety of PCSK9 inhibitors
Most importantly, PCSK9 inhibitor antibodies cannot cross the blood-brain barrier, so they don’t directly affect brain cholesterol levels
Genetic evidence:
Large-scale Mendelian randomization studies across 740,000 participants found that genetically proxied PCSK9 inhibition showed null effects for every cognitive-related outcome tested. However, the average person had high cholesterol in this study so the lower bounds of PCSK9’s inhibition on cholesterol levels may not have been thoroughly tested.
People born with loss-of-function PCSK9 mutations have lifelong very low LDL cholesterol (sometimes as low as 15 mg/dL) with normal cognitive function and no neurological problems
In elderly populations, the protective rs11591147 variant was associated with lower cholesterol but showed no association with cognitive performance or activities of daily living
PCSK9 in Alzheimer’s Disease: An Emerging Story
Recent research suggests PCSK9 may play roles in Alzheimer’s disease beyond cholesterol:
Brain autopsies of Alzheimer’s patients show elevated PCSK9 levels in the frontal cortex
Preclinical studies suggest PCSK9 inhibition may enhance clearance of amyloid-β peptides across the blood-brain barrier
These findings raise an exciting possibility: that PCSK9 inhibitors (if they were designed to cross the blood-brain barrier) might offer neuroprotection through mechanisms beyond cholesterol lowering. However, this remains speculative and requires long-term outcome studies to confirm.
The Clinical Actionability of PCSK9 Genetics
So how can you use genetic information about PCSK9 variants clinically?
Risk Stratification
While individual PCSK9 variants have modest effects, they contribute valuable information:
High-risk variants (rs505151 G allele): May warrant earlier lipid screening, more aggressive treatment targets, and earlier consideration of PCSK9 inhibitor therapy
Protective variants (rs11591147 T allele): Provide reassurance that low cholesterol goals are safe and may inform less aggressive treatment approaches
Polygenic risk scores: The most actionable approach—combining PCSK9 variants with hundreds of other genetic markers to create a comprehensive cardiovascular risk profile
Personalized Treatment Decisions
Genetic risk stratification is particularly valuable for PCSK9 inhibitor therapy because:
These drugs are expensive ($4,000-6,500 annually)
Insurance often requires extensive prior authorization
Not everyone benefits equally
High polygenic risk score patients derive 2-3 times greater benefit than lower-risk patients
In the ODYSSEY OUTCOMES trial, patients with high polygenic risk scores experienced 37% relative risk reduction with alirocumab versus only 13% in lower-risk patients. This kind of precision medicine approach helps justify the cost and optimize patient selection.
Family Cascade Screening
If you’re found to have gain-of-function PCSK9 mutations causing familial hypercholesterolemia:
First-degree relatives have a 50% chance of carrying the same mutation
Early identification through cascade screening allows preventive treatment before cardiovascular damage occurs
Genetic testing is now recommended for all suspected familial hypercholesterolemia cases
PCSK9 Inhibitors: From Discovery to Market
The development of PCSK9 inhibitors represents one of the fastest translations from genetic discovery to FDA approval in pharmaceutical history.
Timeline of Development
2003: PCSK9 identified as cause of familial hypercholesterolemia
2006: Loss-of-function variants shown to reduce cardiovascular disease by 88%
2015: FDA approves alirocumab (Praluent) and evolocumab (Repatha)—the first PCSK9 inhibitors
2021: FDA approves inclisiran (Leqvio)—a next-generation siRNA therapy
2024: FDA expands inclisiran indications for primary prevention
2025-2026: Expected approval of lerodalcibep and potentially oral PCSK9 inhibitors
Just 12 years from gene discovery to approved therapy—an unprecedented achievement.
Currently Available PCSK9 Inhibitors
First Generation: Monoclonal Antibodies
Evolocumab (Repatha, Amgen) and Alirocumab (Praluent, Sanofi/Regeneron)
FDA approved: July-August 2015
Mechanism: Fully human monoclonal antibodies that bind PCSK9 and prevent it from degrading LDL receptors
Administration: Subcutaneous injection every 2-4 weeks
LDL-C reduction: 50-60%
Cardiovascular risk reduction: 15-20% in outcome trials (FOURIER and ODYSSEY)
Cost: $5,800-6,500 annually (down from $14,000 at launch)
A third monoclonal antibody, bococizumab (Pfizer), was discontinued due to immunogenicity issues—highlighting the importance of fully human versus humanized antibodies.
Second Generation: siRNA Therapy
Inclisiran (Leqvio, Novartis)
FDA approved: December 2021
Mechanism: Small interfering RNA that silences PCSK9 mRNA production in liver cells
Administration: Subcutaneous injection at 0, 3 months, then every 6 months
LDL-C reduction: 50-52%
Unique advantage: Twice-yearly dosing improves adherence
Cost: $9,750 first year, $6,500 annually thereafter
Must be administered by healthcare provider (not self-injected)
The twice-yearly dosing of inclisiran is revolutionary for patients struggling with adherence or injection fatigue.
PCSK9 Inhibitors in Development
The pipeline is rich with innovations:
Third Generation: Next-Wave Biologics
Lerodalcibep (LIB003, LIB Therapeutics)
Expected FDA approval: Early 2026
Mechanism: Small recombinant fusion protein combining PCSK9-binding domain with human serum albumin
Administration: Once-monthly subcutaneous injection in small volume (1.2 mL)
LDL-C reduction: 56-69% in phase 3 trials
Key advantages: No refrigeration required, stable for 9 months, quick injection (12 seconds)
Over 90% of patients achieved European guideline LDL-C targets
Oral PCSK9 Inhibitors
MK-0616 (formerly enlicitide decanoate, Merck)
Currently in phase 3 trials with outcomes trial planned
LDL-C reduction: Up to 66% in early studies
Formulation with sodium caprate enables higher bioavailability
Would be first oral PCSK9 inhibitor if approved
AstraZeneca oral agent
Earlier in development pipeline
Represents alternative approach to oral PCSK9 inhibition
Other Novel Approaches
PCSK9 vaccines (Vaxxinity): One-time or infrequent vaccination to generate anti-PCSK9 antibodies
Gene editing (VERVE-101, Verve Therapeutics): CRISPR-based one-time treatment to permanently reduce PCSK9 production
Antisense oligonucleotides (AZD8233, AstraZeneca/Ionis): Alternative approach to reduce PCSK9 mRNA
Small molecule transcriptional inhibitors: Early-stage compounds that reduce PCSK9 gene expression
The goal of these next-generation approaches? Less frequent dosing, oral administration, and potentially one-time treatments.
Who Should Take PCSK9 Inhibitors vs. Statins?
This is the practical question for patients and clinicians.
Statins Remain the Foundation
Statins are still first-line therapy for virtually all patients requiring cholesterol lowering. PCSK9 inhibitors are add-on therapy, not replacements.
The treatment paradigm follows a step-wise approach:
Start with maximally tolerated statin therapy
Add ezetimibe if not at LDL-C goal
Consider PCSK9 inhibitor if still not at goal despite steps 1-2
2022 ACC/NLA Guidelines: Who Qualifies for PCSK9 Inhibitors?
Based on the latest American College of Cardiology and National Lipid Association guidelines:
Secondary Prevention (Established Cardiovascular Disease)
Very High-Risk Patients:
Multiple major cardiovascular events OR one major event plus multiple high-risk conditions
LDL-C ≥55 mg/dL despite maximally tolerated statin (and typically ezetimibe)
PCSK9 inhibitor is “reasonable” to add
Not-at-Very-High-Risk Patients:
Established cardiovascular disease
LDL-C ≥70 mg/dL despite maximally tolerated statin
PCSK9 inhibitor is “reasonable” to add
Primary Prevention (No Cardiovascular Disease Yet)
Familial Hypercholesterolemia:
Diagnosed heterozygous familial hypercholesterolemia
LDL-C ≥100 mg/dL despite maximally tolerated statin plus ezetimibe
Age 30-75 years
PCSK9 inhibitor should be considered
Severe Primary Hypercholesterolemia:
LDL-C ≥190 mg/dL at baseline (without genetic diagnosis of FH)
LDL-C remains ≥100 mg/dL on maximally tolerated statin plus ezetimibe
Multiple cardiovascular risk factors present
PCSK9 inhibitor may be considered
Statin Intolerance
Clinical cardiovascular disease OR baseline LDL-C ≥190 mg/dL
Unable to tolerate statins despite trying multiple formulations
PCSK9 inhibitor may be considered
Special Populations Where PCSK9 Inhibitors Show Particular Benefit
Peripheral Artery Disease:
In the FOURIER trial, patients with lower limb PAD had 42% reduction in major adverse limb events with evolocumab
Similar results in ODYSSEY OUTCOMES with 41% reduction in limb events
This population is often undertreated for cholesterol
Recent Acute Coronary Syndrome:
Patients within months of heart attack or unstable angina
Very high recurrent event risk
Both FOURIER and ODYSSEY trials showed robust benefits in this population
High Polygenic Risk Score Patients:
Even with average LDL-C levels clinically
May derive outsized benefit from intensive LDL lowering
Emerging use of genetic testing to identify these patients
Practical Considerations
Prior Authorization: Insurance companies typically require documentation of:
Diagnosis (ASCVD, familial hypercholesterolemia, etc.)
Current LDL-C level despite maximally tolerated statin
Trial of ezetimibe (in most cases)
Patient-specific risk factors
Cost and Value: At current prices ($4,000-6,500 annually for monoclonal antibodies), PCSK9 inhibitors are most cost-effective when targeted to very high-risk patients. For patients in the top percentiles of cardiovascular risk (based on clinical factors and potentially genetic risk scores), the benefit clearly outweighs the cost.
Natural PCSK9 Inhibitors: Recent Evidence
Contrary to earlier assumptions, emerging research has identified several natural compounds that can modulate PCSK9 levels. While these supplements don’t replace pharmaceutical PCSK9 inhibitors for high-risk patients, they represent promising adjunct approaches for cardiovascular health.
Berberine: The Most Potent Natural PCSK9 Inhibitor
Berberine, an alkaloid found in several plants including goldenseal and barberry, has demonstrated PCSK9-lowering effects:
Mechanism: Berberine inhibits PCSK9 transcription by inducing proteasomal degradation of hepatocyte nuclear factor 1a (HNF1a), a key transcription factor for PCSK9 expression.
Research findings: In cell studies: 77% reduction in PCSK9 mRNA and 87% reduction in PCSK9 protein levels. In animal studies: 50% reduction in serum PCSK9 levels in high-fat diet mice after 16 days of treatment. Clinical trials: Formulations containing berberine (500mg) reduced LDL-C by 20-50 mg/dL across multiple studies
Practical considerations: Typical dosage: 500mg, 2-3 times daily with meals. May cause gastrointestinal side effects. Can interact with various medications including diabetes drugs.
Curcumin: Synergistic with Statins
Curcumin, the active compound in turmeric, works through a similar but distinct mechanism to berberine:
Mechanism: Curcumin reduces nuclear abundance of HNF1a, leading to downregulation of PCSK9 gene expression. Importantly, it decreases statin-induced PCSK9 expression, potentially enhancing statin efficacy.
Research findings: Cell studies: Downregulates PCSK9 at transcriptional level while increasing LDL receptor expression. Human study: Micellar curcumin (105 mg/day for 7 days) reduced PCSK9 concentrations by approximately 10% in healthy volunteers.
Practical considerations: Standard curcumin has poor bioavailability. Micellar or liposomal formulations show 14-39 fold better absorption. Typical dosage: 500-1000mg daily of enhanced bioavailability formulations. Generally well-tolerated with minimal side effects.
Omega-3 Fatty Acids (EPA and DHA)
High-dose omega-3s, particularly EPA (eicosapentaenoic acid), affect PCSK9 levels:
Research findings: EPA + DHA supplementation showed inverse correlation with plasma PCSK9 changes (r = -0.52, p =0.041) in subjects with high apolipoprotein B. The landmark REDUCE-IT trial using 4g daily of pure EPA showed 25% reduction in cardiovascular events. Effects appear dose-dependent: therapeutic doses of 2-4g daily show cardiovascular benefits.
Practical considerations: For PCSK9 effects, higher doses (2-4g EPA+DHA daily) may be needed. Pure EPA (icosapent ethyl) showed better cardiovascular outcomes than EPA/DHA combinations. Choose pharmaceutical-grade omega-3s to avoid contaminants. May increase bleeding risk when combined with blood thinners.
Hot tip: I personally eat a handful of walnuts per day, which has a daily serving of Omega-3s. Studies have shown that dietary consumption of Omega-3 is superior to taking a supplement for cardiovascular disease.
Standard Lipid-Lowering Lifestyle
These evidence-based approaches work through complementary mechanisms:
• Mediterranean diet: Rich in polyphenols, omega-3s, and fiber
• Regular aerobic exercise: 150+ minutes weekly
• Weight management: Particularly visceral fat reduction
• Smoking cessation: Critical for vascular health
These lifestyle factors lower LDL cholesterol and reduce cardiovascular risk through multiple pathways, including but not limited to PCSK9 modulation.
For Those with High Genetic Risk:
If your NeuroAge genetic testing reveals you carry high-risk PCSK9 variants or high polygenic risk scores for cardiovascular disease:
Be proactive about lipid screening starting in your 20s or 30s
Work with your physician to optimize statin therapy early
Consider more aggressive LDL-C targets than standard guidelines
If PCSK9 inhibitor therapy is recommended, prioritize obtaining it—the genetic data can actually help with insurance approval
Future Directions and Staying Updated
The PCSK9 field continues to evolve rapidly:
Near-term (2025-2026):
Lerodalcibep likely approval
Expanded real-world evidence for inclisiran
Potential approval of oral PCSK9 inhibitors
Medium-term (2027-2030):
PCSK9 vaccine approaches may reach late-phase trials
Gene editing approaches (VERVE-101) moving through trials
Potentially broader insurance coverage as competition increases prices
Long-term Questions:
Will long-term (decades) PCSK9 inhibition prove safe for non-cardiovascular outcomes?
Can we identify patients who benefit from PCSK9 inhibition beyond cholesterol lowering (e.g., for neuroprotection)?
Will one-time gene editing approaches become the standard of care?
Conclusion
The PCSK9 story beautifully illustrates the power of human genetics to transform medicine. From the initial discovery in 2003 to multiple approved drugs just 12-15 years later, PCSK9 inhibitors represent a triumph of translational research.
Key takeaways:
On Genetics:
PCSK9 variants rs505151 and rs11591147 meaningfully affect cardiovascular risk and longevity
Polygenic risk scores incorporating PCSK9 variants can identify patients who benefit most from intensive treatment
Genetic information is actionable—it helps guide treatment decisions and family screening
On Brain Health:
Despite profound LDL cholesterol lowering, PCSK9 inhibitors appear safe for cognition
People born with lifelong low cholesterol due to PCSK9 mutations have normal brain function
Intriguing early evidence suggests PCSK9 inhibition might have neuroprotective effects beyond cholesterol
On Treatment:
PCSK9 inhibitors are powerful add-on therapies for high-risk patients not at goal with statins
Current options include twice-monthly, monthly, and twice-yearly injectable formulations
Oral formulations are on the horizon
Cost remains a barrier but is decreasing as competition increases
On Longevity:
Genetic evidence links lower PCSK9 activity to extended lifespan (particularly in men, approximately 2.4 years per standard deviation LDL-C reduction)
The effect appears to work primarily through cardiovascular disease prevention
High-quality polygenic risk scores may become standard tools for personalized preventive cardiology
Whether you’re managing your own cardiovascular risk, interpreting genetic testing results, or simply curious about cutting-edge preventive medicine, PCSK9 represents one of the most important therapeutic targets of our time—and the story is still being written.
If you’ve had your genetics analyzed through NeuroAge, check your PCSK9 variant status and discuss the implications with your healthcare provider. Understanding your genetic risk profile can inform more personalized and effective prevention strategies.
Stay tuned for updates as oral PCSK9 inhibitors, vaccines, and gene editing approaches progress through clinical development.

Written by
Dr. Christin Glorioso, MD PhD
Dr. Glorioso is the founder and CEO of NeuroAge Therapeutics. With her background in neuroscience and medicine, she is dedicated to revolutionizing brain health and helping people maintain cognitive vitality.
Learn more about Dr. Glorioso

