
Optimal cholesterol levels for longevity and brain health
Making sense of the wide range of opinions on ideal cholesterol levels
Surprisingly, the ideal cholesterol level range is controversial even today.
Dr. Peter Attia in his recent New York Times bestselling book, Outlive, recommends LDL levels <70 mg/dl with the ideal being an outlandish (in my opinion) 10-20 mg/dl. It’s worth noting that Attia has heart disease in his family so this aggressive approach may be optimized for preventing coronary events.
On the other hand, I have recently heard other self-described experts in the space recommend higher cholesterol levels, much higher, than the American Heart Association (AHA) guidelines. Some functional medicine physicians are also warning against statin use, which is surprising to me. Multiple consumers have told me that “you need cholesterol for the brain” and are wondering how to lower body cholesterol while retaining brain cholesterol levels.
So why do we have so many radically different opinions about a basic and well-established biomarker? I decided to dive in to try and get to the bottom of it and make sure that I am making the best decisions for my own health.
First, the AHA guidelines:
”While there is no ideal target level for LDL-C, the 2018 guideline recognizes that “lower is better.” Studies suggest that:
Optimal total cholesterol is about 150 mg/dL
Optimal LDL-C is at or below 100 mg/dL. Adults with LDL-C in this level have lower rates of heart disease and stroke”
The AHA is primarily concerned with cardiovascular health, though. For cardiovascular health, lower is consistently better across studies although it plateaus around a total cholesterol of 180 mg/dL.

What about all cause mortality?
This is where some of the controversy stems from.
According to one large recent study in a Korean population, there is a U-shaped curve for all cause mortality with ideal levels being between 200-250 (see figure below).
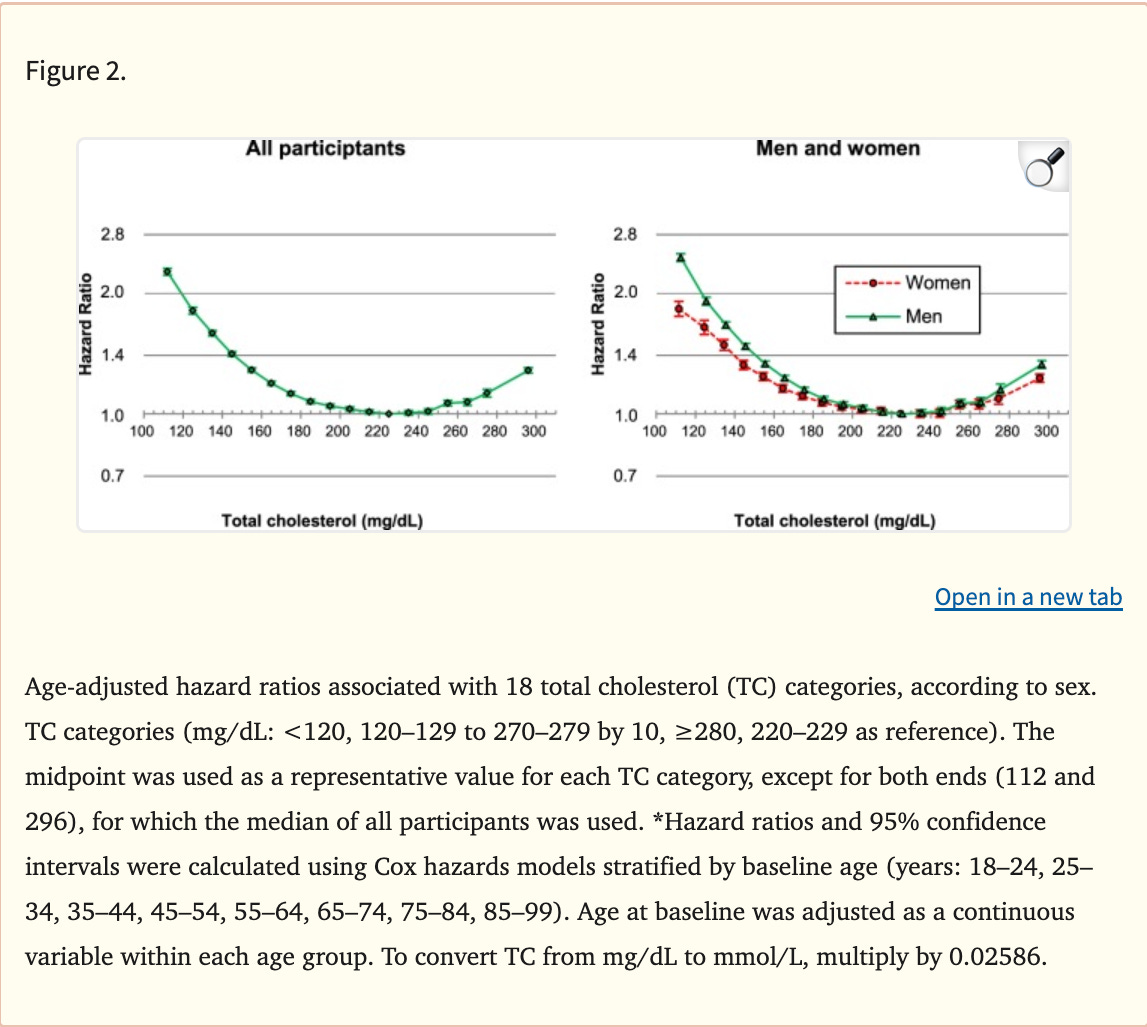
This is not true of every study examining mortality vs. cholesterol level. Furthermore, if you break it down by age group, you can see that the ideal cholesterol level is lower in younger people.
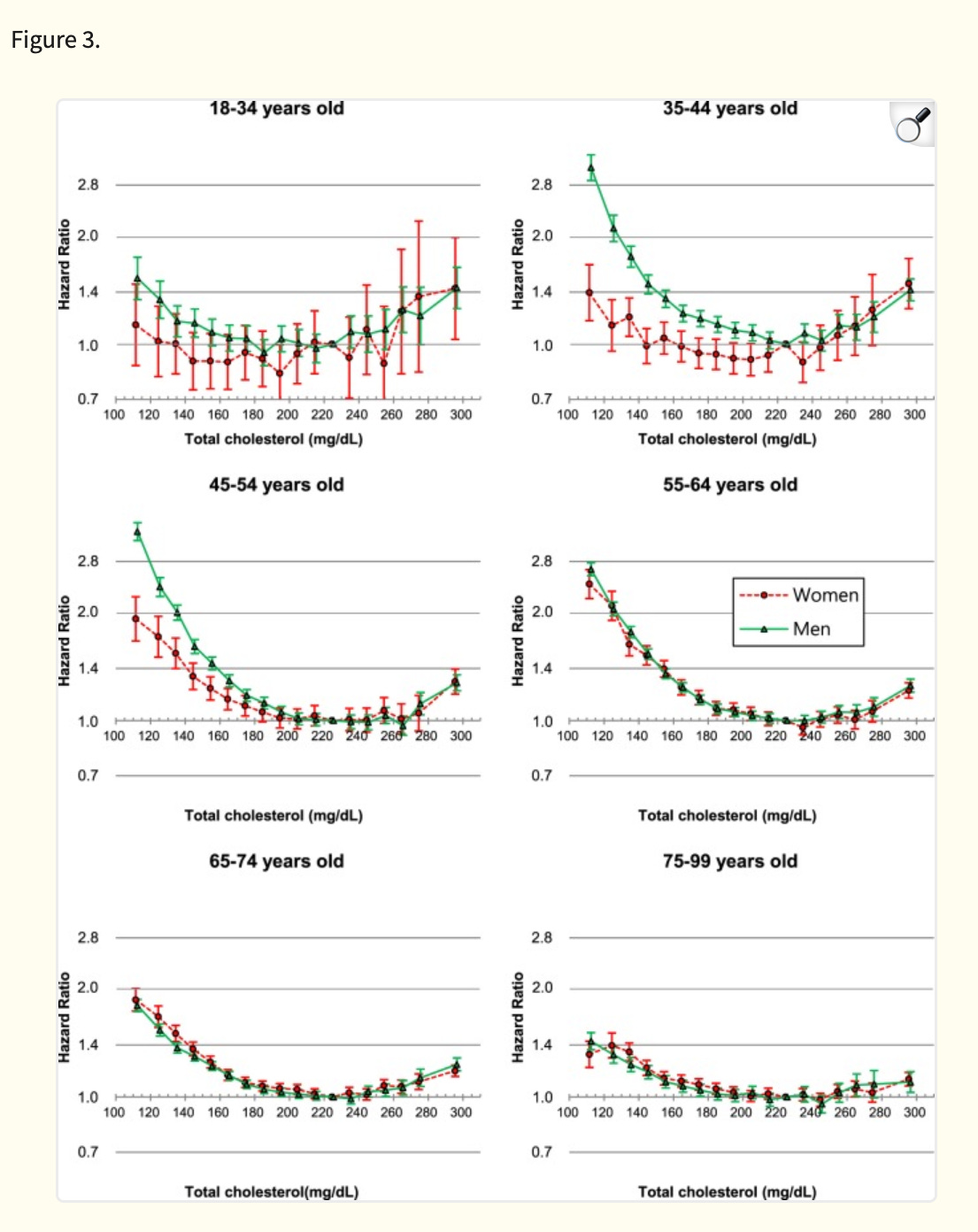
In mid life or younger in this study, the ideal total cholesterol level is closer to 200. However, both the young and old extremes of age see a “flattening” of the relationship between cholesterol levels and mortality. This is likely due to confounding factors that I describe in more detail below.
What about risk of other diseases?
If you look at the cancer and dementia risk literature, you also see that seemingly optimal cholesterol levels are higher than the AHA recommendations in older age— 200-240 is ideal in older folks for dementia risk and 160-220 is ideal for cancer risk.
There are some important confounders to point out with these correlative studies. For dementia a drop in cholesterol can signal onset of disease. This is largely due to a lack of proper nutrition, which results in lower cholesterol levels. The low cholesterol is not causing the dementia but is instead a consequence of it.
Similarly, cancer can physiologically cause a drop in cholesterol levels. Studies have shown this both in mice and in people.
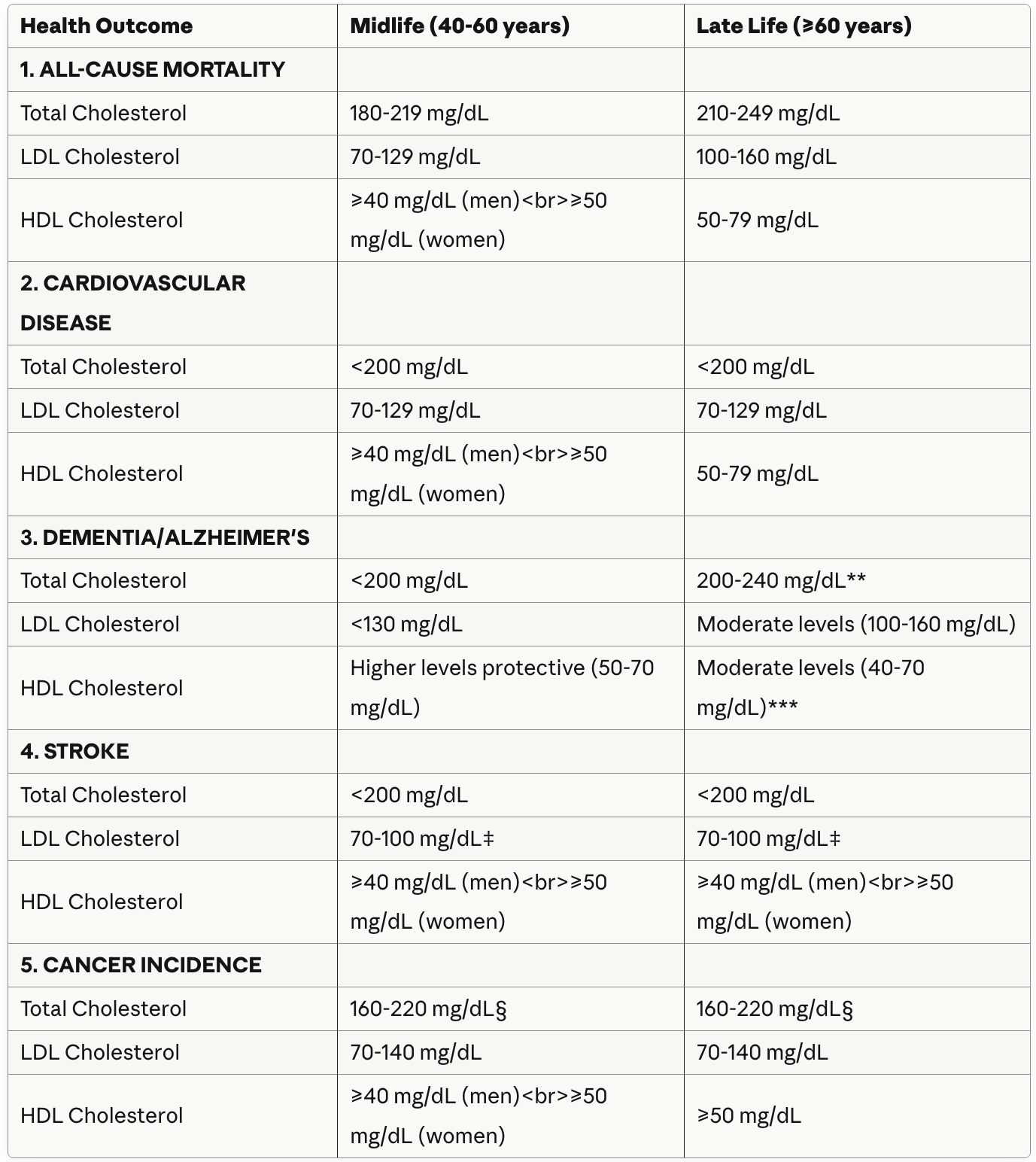
Below you can see a summary of the optimal levels of total, LDL, and HDL (“good cholesterol”) by age and by health outcome in the best large correlative studies.
Important Clinical Notes
† Late-Life Cholesterol: In adults >75 years, declining cholesterol levels may reflect underlying disease processes rather than being causally related to outcomes. Treatment decisions should be individualized.
‡ Stroke Prevention Balance: Very aggressive LDL lowering (<70 mg/dL) reduces ischemic stroke but may slightly increase hemorrhagic stroke risk, particularly in those with uncontrolled hypertension.
§ Cancer and Cholesterol: Very low cholesterol (<160 mg/dL) associated with cancer is primarily reverse causation—undiagnosed cancer lowers cholesterol 2-5 years before diagnosis. Studies excluding early cancers show minimal long-term association. Low HDL (<40 mg/dL) independently predicts multiple cancer types.
** Late-Life Dementia Paradox: The relationship reverses in late life. Higher cholesterol in older adults (age 70-88) was associated with 23-30% reduced dementia risk, though high cholesterol still increases AD-specific risk. This likely reflects that very low cholesterol in elderly signals frailty, malnutrition, or preclinical disease. Moderate levels (200-240 mg/dL) appear optimal.
*** HDL and Late-Life Dementia: While higher HDL is protective in midlife, extremely high HDL (>80 mg/dL) in adults ≥75 years was paradoxically associated with increased dementia risk in the ASPREE cohort. Moderate HDL (40-70 mg/dL) appears optimal across all ages.
Age-Related Changes: Optimal ranges generally shift higher with age for all-cause mortality, though CVD-specific targets remain lower. The strength of cholesterol-mortality associations weakens with advancing age.
Additional evidence: statins and other cholesterol-lowering medications show protective benefits for dementia
I review the positive evidence for use of statins in another article. I will add that in a recent study of ~15,000 people who were on average 80 years old, researchers showed a dose-dependent improvement in memory with the number of years of statin use. Simvastatin was superior to atorvastatin in improving memory.
It should be noted that statins may have additional benefits beyond lowering cholesterol as they affect multiple pathways. Also, not all statins cross the blood brain barrier, which is an important and nuanced factor for choosing which statin to take. I will save the discussion of the best medications for lowering cholesterol for dementia prevention for a future post.
Putting it all together
Balancing all of the information about risk of various diseases, my recommendations are below. These recommendations reflect the cholesterol ranges that best intersect optimal levels for all ages and outcomes.
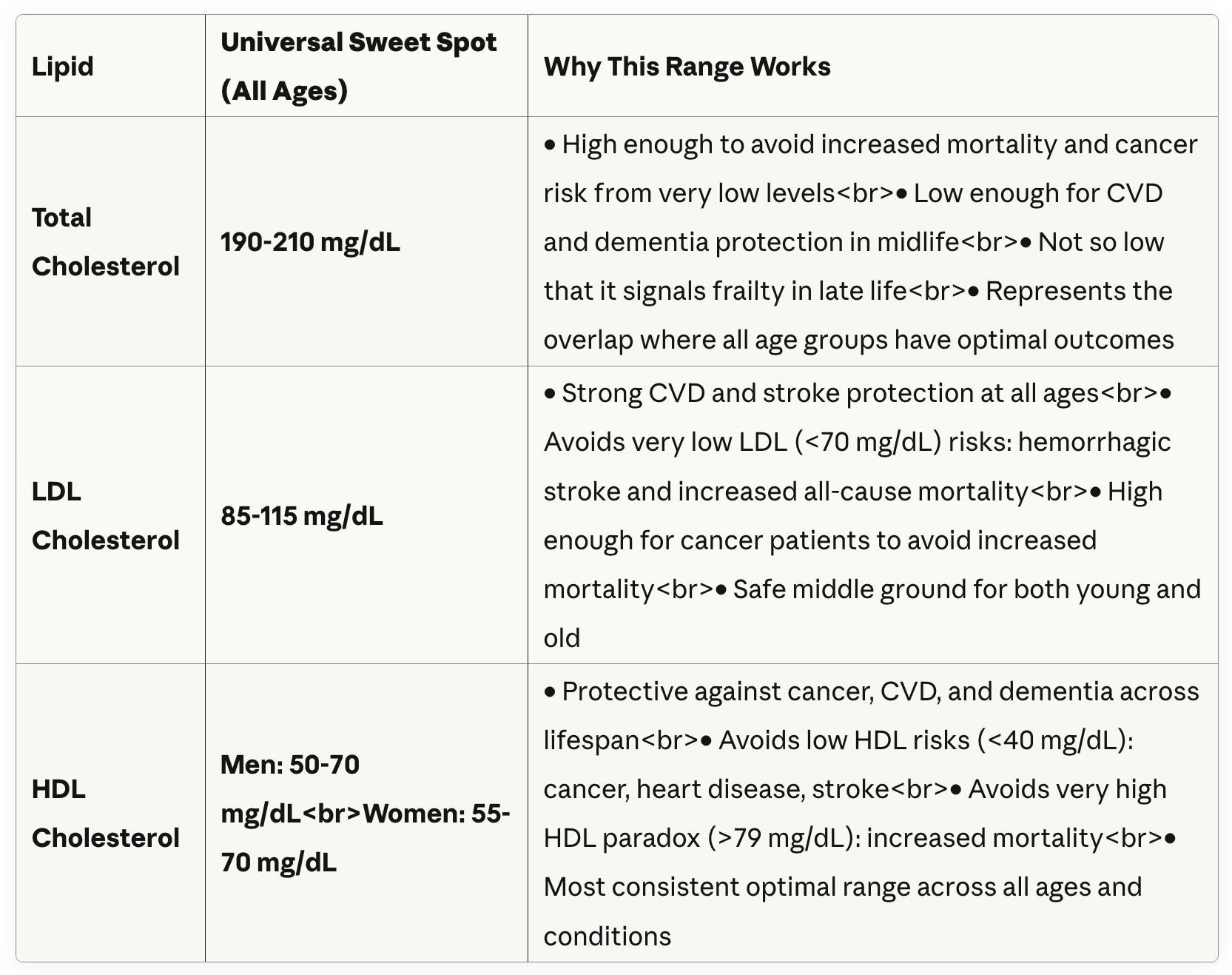
These levels are higher than the levels recommended by Dr. Peter Attia and the AHA but not as high as some functional medicine doctors are recommending. As usual, the best path is often somewhere in the middle.
My recent total cholesterol was 160 mg/dl. This review has prompted me to opt for a slightly lower dose of my statin and aim for closer to 190.
If the higher optimal cholesterol ranges for cancer and dementia probably reflect confounding factors, why not ignore those results and aim for lower levels?
The mortality data in younger people is convincing enough to me and I think there is a high enough chance that some of the signal is real in older folks for dementia that I’d rather split the difference and aim a bit higher than the AHA recommendations.
If heart disease or stroke is the biggest concern for an individual based on their own medical or family history or genetic risk factors, aiming lower might make sense.

Written by
Dr. Christin Glorioso, MD PhD
Dr. Glorioso is the founder and CEO of NeuroAge Therapeutics. With her background in neuroscience and medicine, she is dedicated to revolutionizing brain health and helping people maintain cognitive vitality.
Learn more about Dr. Glorioso

