
How Much Protein Does Your Brain Actually Need?
Making sense of conflicting data and a sample meal plan for APOE4 carriers

People ask me about protein all the time. How much should I eat? Is plant protein really better? Should I be worried about mTOR? And increasingly, does my APOE4 status change the answer?
I’ve been diving deep into this literature, both for NeuroAge’s research and for my own health. As an APOE4 carrier who follows a mostly Mediterranean diet, I have a personal stake in getting this right. And the evidence is more complicated than most people in the longevity space make it sound.
The Conflicting Data
There is tension at the core of the protein-and-brain-health literature. Two bodies of evidence point in opposite directions, one is from human observational data and one is from animal data.
For the brain especially, I’m very skeptical of the mouse literature. Mouse brains age differently than human brains and mice don’t suffer from dementia in the way that we humans do. This means that I don’t put a lot of weight on the data on low protein and mouse lifespan that is commonly pointed to in the longevity community but I do take it into account as something to be aware of.
The best quality data would be from randomized control trials (RCTs) or at least mendelian randomization (MR) studies, neither of which we have. If you read my post on alcohol and the brain, you know how different the results of observational studies can be from causal human studies. Here I put together what we know so far in the absence of more rigorous information.
The human observational data says: more protein, better cognition
The largest study comes from Yeh et al. (2022) in the American Journal of Clinical Nutrition, which followed over 77,000 participants from the Nurses’ Health Study and Health Professionals Follow-up Study for more than 20 years. Their findings were striking. For every 5% of calories that came from plant protein instead of carbohydrates, there was a 26% lower risk for developing cognitive decline. For animal protein replacing carbs, the risk reduction was 11%. Beans and legumes had the strongest protective association, with peas and lima beans linked to a 28% lower risk of cognitive decline for every additional three servings per week.
A systematic review and meta-analysis of nine studies totaling nearly 5,000 older adults confirmed the pattern. Higher protein intake was consistently associated with better cognitive functioning. The proposed mechanism involves branched-chain amino acids (BCAAs) crossing the blood-brain barrier and supporting glutamate synthesis in brain areas dedicated to learning and memory, a process that becomes increasingly important with age.
And there’s the muscle connection, which I think is under-appreciated. Burns et al. showed that individuals with early-stage Alzheimer’s had decreased lean muscle mass, and that reductions in white matter volume, whole brain volume, and cognitive performance were all significantly associated with reduced lean mass.
Of course, we should be very careful in conflating correlation with causation. People who are suffering from Alzheimer’s disease also are less likely to take care of themselves including being less likely to engage in resistance training, leading to reverse causation. The Alzheimer’s could be causing people to have less lean muscle mass, not the other way around.
The animal and mechanistic data says: less protein, slower brain aging
On the other side, we have some of the most elegant work in aging biology. Lamming et al. (2024) in Nature Communications showed that protein restriction in the 3xTg Alzheimer’s mouse model reduced AD pathology, decreased mTORC1 activity, increased autophagy, improved cognition, and extended survival. This is a clean, well-controlled study. The mechanism is straightforward. Dietary amino acids activate mTORC1, which inhibits autophagy, which is the cellular cleaning process responsible for clearing the damaged proteins that accumulate in Alzheimer’s.
A separate study using APP knock-in mice confirmed that reducing dietary protein promoted autophagy and prevented amyloid plaque deposition. And Longo’s work using the Geometric Framework showed that mice on 5-15% protein diets lived up to 150 weeks compared to 100 weeks for those on ~50% protein, despite the higher-protein mice being leaner. Protein restriction also reduced IGF-1 and tau phosphorylation in the hippocampus.
If you’ve read my mTOR article, you know I think this pathway is central to brain aging. But as I wrote there, “it’s not simply about maximizing or minimizing any single pathway, but rather about finding the right balance for your individual biology.”
So How Many Grams, Actually?
The Longo camp (longevity-first): Valter Longo recommends 0.31 to 0.36 grams per pound of body weight for adults under 65, which works out to about 0.68-0.8 g/kg. After 65, he recommends increasing slightly to about 1 g/kg to prevent sarcopenia and frailty. His reasoning is rooted in the GH/IGF-1 pathway data. His research shows that Americans getting 20% or more of their daily calories from protein had nearly 400% higher cancer rates compared to those at 10% of calories from protein, along with a 75% increase in overall mortality. But this association reversed after age 65, where higher protein became protective.
The Phillips/muscle camp (function-first): Stuart Phillips at McMaster recommends roughly double what Longo suggests: 1.2-1.6 g/kg for younger adults and even higher for older adults. Kara Fitzgerald’s synthesis lands at 1.2-1.6 g/kg for younger adults and 1.5-2.2 g/kg for older folks.
The RDA baseline: The government’s recommended dietary allowance is 0.8 g/kg, which was designed to prevent deficiency in a 25-year-old male. Most experts agree this is inadequate for older adults or active individuals.
In my IGF-1 article, I recommended a protein intake of 1.0-1.2 g/kg alongside resistance training, sleep optimization, and reducing chronic inflammation. I still think that’s a reasonable middle ground for most people, but the nuance matters a lot depending on your age, activity level, and genetics.
The Source Matters More Than the Quantity
If I’ve learned one thing from this deep dive, it’s that the type of protein may matter more than the total grams.
The Yeh et al. Harvard data showed plant protein was more than twice as protective as animal protein for cognitive decline (26% vs. 11% risk reduction per 5% caloric substitution). Plant-based protein foods also have the lowest amounts of advanced glycation end products (AGEs), which are inflammatory compounds that accumulate with age and contribute to neurodegeneration.
A Chinese cohort study following community-dwelling older adults over 9 years found that fish protein intake was independently associated with lower risk of cognitive decline, consistent with a prior study showing that one or more servings of fish per week reduced the cognitive decline rate in adults over 65. An adequate methionine status from animal foods may also decrease risk of dementia and brain atrophy. So this isn’t a simple animal-bad, plant-good story.
What does seem harmful is processed meat and high-methionine, high-saturated-fat protein sources. The macronutrient-cognition review in Clinical Nutrition found that saturated fatty acid intake consistently correlates with decreased memory and learning scores, while omega-3 intake correlates positively with memory. The protein itself isn’t the villain. It’s what comes packaged with it.
This is why I try to choose seafood, chicken, or plants as my protein sources and mostly avoid red meat, highly processed and fried foods, and sugary drinks. As I’ve written before, I eat at least 6 walnuts a day and try to choose seafood as my protein source whenever possible. The upside to eating brain healthy foods is that you don’t have much room left for junk food.
What APOE4 Carriers Need to Know
A 2024 study in Alzheimer’s Research & Therapy (Keum et al.) is one of the first to directly test the interaction between protein intake and APOE4 status on cognition. In 196 older adults without dementia, high protein intake was significantly associated with better episodic memory and overall cognition. But the key finding was a significant interaction between high protein intake and APOE4 status, meaning that APOE4 moderated the association between protein and episodic memory. In other words, the cognitive benefit of higher protein appeared stronger in E4 carriers.
A separate longitudinal cohort study concluded that diversified protein food intake combined with frequent fish consumption may reduce the detrimental effect of APOE4 on cognitive health.
However, there’s a critical caveat. The Three-City cohort study found that the inverse association between fish consumption and dementia was seen only among APOE4 non-carriers. The PreventE4 trial at USC (Yassine group) should give us important answers.
My read on this for E4 carriers is to get your protein, prioritize plant sources and fish, but be strategic about your omega-3 delivery form. And restrict saturated fat, which in E4 carriers is associated with up to a 7-fold increased risk of Alzheimer’s compared to non-carriers eating the least saturated fat.
The Age-Dependent Switch
One important concept in the protein literature is that the optimal intake likely changes with age, and the inflection point appears to be somewhere around 65.
Before 65, the evidence from Longo and others suggests that moderate protein restriction (0.8-1.0 g/kg) may be beneficial by keeping mTOR/IGF-1 signaling in check, promoting autophagy, and reducing cancer risk. Longo’s own studies showed that higher protein amounts were better for people over 65 but not optimal for those under 65. His 2022 Cell paper described the longevity diet as having moderate to high carbohydrate intake from non-refined sources, low but sufficient protein from largely plant-based sources, and enough plant-based fats to provide about 30% of energy needs.
After 65, the equation supposedly flips. Sarcopenia becomes a major risk factor for cognitive decline. The Burns et al. data linking lean mass to brain volume is hard to ignore. And the review in Frontiers in Nutrition notes that reduced absorption of key nutrients, including proteins, is common in the elderly due to atrophic gastritis and declining metabolic rate. Population-based studies indicate that the risk of dementia is significantly reduced among individuals adhering to a diet with a high percentage of caloric intake from protein sources in this age group.
For those of us in midlife, this creates a tension. We want to keep mTOR in check and promote autophagy. But we also need to maintain muscle mass, which is protective for the brain. My personal approach is moderate protein (roughly 1.0-1.2 g/kg) with most coming from plant and fish sources, combined with regular resistance training.
A Note on the Evidence Quality
The strength of the evidence behind these protein recommendations is much weaker than people assume. If you’ve been reading my Substack for a while, you know I care about distinguishing what we know from what we think we know. So let’s talk about study design.
We have almost no RCTs.
The vast majority of the protein-cognition literature consists of observational studies, primarily prospective cohorts like the Nurses’ Health Study. These are valuable, but they cannot prove causation. People who eat more plant protein also tend to exercise more, smoke less, have higher incomes, and follow healthier overall dietary patterns. Statistical adjustments help, but they can never fully eliminate confounding.
A 2024 systematic review of RCTs examining dietary protein interventions and cognitive function in adults found that the evidence from individual RCTs is “less consistent” than what observational studies suggest. Improvements were observed in only three out of nine studies evaluating psychomotor speed, and many of the positive findings on memory came from nut interventions specifically, making it hard to disentangle the protein effect from other bioactive compounds in nuts (polyphenols, healthy fats).
One 2024 RCT tested 15g/day of whey protein powder for 12 months in older adults with mild cognitive impairment. The whey protein group showed a mean MoCA improvement of 3.23 points compared to 1.42 in the control group. This is encouraging, but it’s a single small trial of a specific protein form in a specific population, and the control received a placebo rather than an equivalent amount of carbohydrate or fat calories.
A Japanese RCT tested seven essential amino acids (3g or 6g daily) in 105 participants over 55. The higher dose group showed improved attention and cognitive flexibility compared to placebo. Again, promising, but small and short-term.
No RCT has tested different total protein intake levels (say, 0.8 vs. 1.2 vs. 1.6 g/kg) head-to-head for cognitive outcomes over multiple years. This is the study we actually need, and it doesn’t exist.
We have no relevant Mendelian randomization data on protein intake and dementia.
Mendelian randomization (MR) uses genetic variants as instrumental variables to test whether an exposure (like protein intake) causally affects an outcome (like dementia risk). It’s one of the best tools we have for causal inference from observational data. I’ve evaluated MR evidence extensively in my articles on IGF-1 and other topics.
But for protein intake and cognitive decline specifically, MR studies essentially don’t exist. Dietary MR is inherently harder than, say, lipid MR, because the genetic instruments for dietary intake are weak and pleiotropic (they influence many things simultaneously, not just what you eat).
There are MR studies on specific dietary habits and AD risk (one 2024 Frontiers study found that oily fish intake was causally protective).
But these are testing different questions than “does eating more or less dietary protein cause dementia.”
What this means for how much to trust the numbers.
The absence of high quality RCT and MR evidence doesn’t mean the observational findings are wrong. It means we should hold our specific numerical recommendations with appropriate humility. When I say “aim for 0.8-1.2 g/kg,” I’m giving you my best synthesis of imperfect evidence, not a proven prescription.
The general direction (adequate protein from diverse plant and fish sources is good for the aging brain) is probably right. But the precise gram targets, the exact magnitude of risk reduction, and the specific mechanisms are far less certain than anyone in the longevity space wants to admit.
This is why I keep coming back to dietary patterns rather than single macronutrient targets. The evidence for Mediterranean-style eating is the most robust across study designs, even if no single component of that pattern has been definitively proven causal through an RCT.
The Big Picture
No clinical trial has ever tested precise macronutrient ratios head-to-head for brain outcomes over 5+ years.
A finding from the FINGER trial cohort showed that a lower carbohydrate-to-fat ratio was associated with better global cognition in older adults at dementia risk. It’s not just about protein, however. The whole dietary pattern matters. Complex carbohydrates over simple ones, unsaturated fats (especially omega-3s) over saturated, plant proteins and fish over processed meats, and quality within each macro category over hitting exact numerical targets.
When people ask me what to eat for brain health, my answer has always been fundamentally simple, even if the science behind it is complex. Eat real food. Mostly a variety of fruits and vegetables. Include fish. Cook with olive oil. Eat berries and nuts. And don’t eat too much. The basics work.
My Practical Takeaways
Here’s where I land for most people focused on brain health:
For adults under 65: Aim for approximately 0.8-1.2 g/kg of protein daily. Emphasize legumes, nuts, seeds, and fish as your primary sources. Include 2-3 servings of low-mercury fish per week. Minimize red and processed meat. Pair with resistance training to maintain lean mass.
For adults over 65: Increase to approximately 1.2-1.6 g/kg, adding more fish, eggs, poultry, and dairy. The priority shifts from mTOR suppression to preventing sarcopenia and frailty, both of which accelerate cognitive decline. Continue resistance training.
For APOE4 carriers at any age: Diversify your protein sources. Plant protein plus regular fish appears especially important. Restrict saturated fat (this is where E4 carriers diverge most from the general population). Be strategic about the quality of your animal protein, keeping saturated fat as low as possible.
For everyone: Quality within each macronutrient category matters more than hitting exact gram targets. A diet of beans, fish, olive oil, vegetables, and berries at slightly “wrong” ratios will massively outperform an optimized macro ratio achieved through protein shakes, processed snacks, and refined carbohydrates.
Putting It All Together: A Sample Day
Theory is nice, but I know most of you want to know what this actually looks like on a plate. So let’s run through a concrete example.
The person: 50 years old, 150 lbs (68 kg), carries one APOE4 allele, exercises about an hour a day, normal BMI, and wants to maintain weight and muscle mass.
The macro framework:
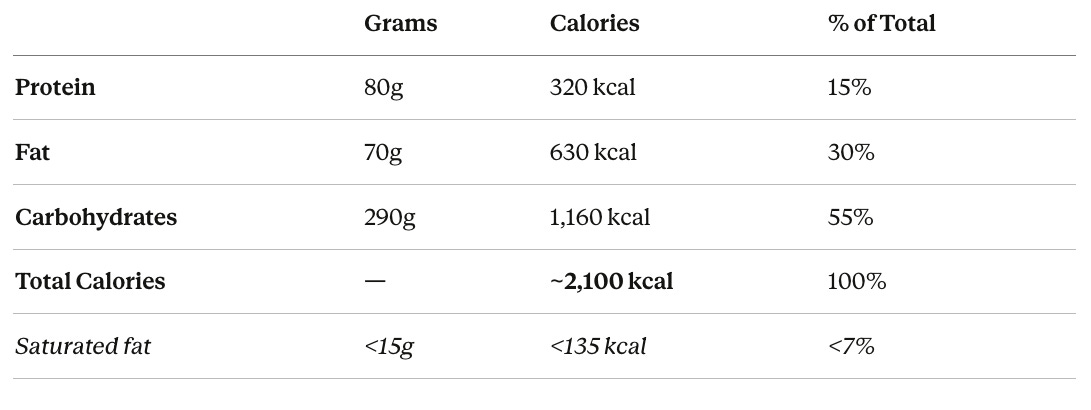
How I arrived at these numbers:
Calories: For a 150 lb person at normal BMI who exercises an hour daily, maintenance falls roughly in the 2,000-2,200 range depending on the type of exercise and baseline metabolism. I’m using 2,100 as a reasonable midpoint.
Protein at 1.2 g/kg (80g): This is the upper end of my general recommendation for someone under 65, and I’m pushing it there for two reasons. First, this person exercises daily and wants to preserve muscle, so they need enough protein to support muscle protein synthesis. Second, the Keum et al. 2024 data suggests that APOE4 carriers may actually get a stronger cognitive benefit from adequate protein than non-carriers. At 80g, we’re well above the inadequate RDA of 0.8 g/kg (54g for this person) but still moderate enough to avoid chronically spiking mTOR and IGF-1 at an age where cancer risk matters.
Fat at 30%: This aligns with the FINGER trial protocol (25-35% from fat), which showed particular cognitive benefit for APOE4 carriers. The critical detail for E4 carriers is keeping saturated fat under 7% of calories. That means the vast majority of those 70g of fat should come from extra virgin olive oil, nuts, seeds, avocado, and fatty fish rather than butter, cheese, or red meat. APOE4 carriers show exaggerated lipid responses to saturated fat compared to non-carriers, and unfavorable lipid profiles are independently associated with greater AD neuropathology.
Carbs at 55%: This is the higher end of the FINGER range, but I want to emphasize that we’re talking about complex, low-glycemic carbohydrates: whole grains, legumes, vegetables, and fruits. Not bread and pasta. The precision nutrition paper for APOE4 highlights that E4 carriers are prone to insulin resistance, so glycemic control matters. If this person tracks their blood glucose and finds they run high despite eating clean carbs, shifting toward a lower-carb, higher-fat approach (with the fat still coming from MUFA and omega-3 sources) would be reasonable.
A sample day:
Breakfast — Berry oatmeal bowl Steel-cut oats cooked in water with oat milk, topped with a cup of mixed berries, a tablespoon of ground flaxseed, and a small handful of chopped walnuts. A cup of black coffee.
~400 kcal | 12g protein | 12g fat | 63g carbs
Lunch — Mediterranean chickpea grain bowl A cup of cooked chickpeas over farro or brown rice, with roasted vegetables (bell peppers, zucchini, red onion), a generous drizzle of extra virgin olive oil, lemon juice, and fresh herbs. Side of mixed greens.
~600 kcal | 20g protein | 18g fat | 90g carbs
Snack — Yogurt with walnuts and honey A cup of unsweetened goat milk yogurt (or plant-based yogurt with live cultures) topped with a few walnut halves and a drizzle of raw honey. A cup of green tea.
~200 kcal | 8g protein | 8g fat | 22g carbs
Dinner — Wild salmon with sweet potato and broccoli Five ounces of grilled or baked wild salmon, one medium sweet potato, steamed broccoli drizzled with a teaspoon of EVOO, and a half cup of quinoa.
~650 kcal | 38g protein | 16g fat | 72g carbs
Evening — Walnuts and dark chocolate A small handful of walnuts (about half an ounce) and a square of 85%+ dark chocolate. ~200 kcal | 4g protein | 14g fat | 10g carbs
Daily approximate total: ~2,050 kcal | 82g protein | 68g fat | 257g carbs
A few things to notice about this day. The protein comes from six different sources (oats, chickpeas, yogurt, salmon, quinoa, walnuts), which is exactly what the research on diversified protein intake and APOE4 protection suggests. The saturated fat is extremely low, probably around 8-10g for the whole day, since the primary fat sources are olive oil, nuts, and fish (goat milk yogurt has less saturated fat than cow’s milk, which is why I chose it here). The omega-3 intake is high between the salmon, walnuts, and flaxseed. The fiber is substantial from all those legumes, whole grains, and vegetables. And the afternoon yogurt isn’t just a snack. Fermented foods deliver live probiotic cultures that directly support the gut-brain axis, which is increasingly recognized as a key player in neuroinflammation and cognitive aging.
Studies show that regular fermented food consumption increases microbial diversity and reduces systemic inflammatory markers like IL-6. For an APOE4 carrier already primed for neuroinflammation, this matters. The coffee and green tea aren’t just for energy either. Both are consistently associated with reduced dementia risk in large cohort studies, likely through their polyphenol content, anti-inflammatory effects, and (in coffee’s case) caffeine’s ability to block adenosine receptors and reduce amyloid-beta accumulation.
Is this day perfect? No. Could you run it through a tracking app and find the carbs are slightly different than my targets? Sure. But that’s the point I keep making. The pattern matters more than the precision. This person is eating real food, mostly plants, with fish, cooked in olive oil, with berries and nuts. The macros fall in a reasonable range. The saturated fat is low. That’s what the evidence actually supports for an APOE4 carrier focused on brain health.
Brain health is a marathon, not a sprint, with decades of small choices adding up to create your lifetime cognitive resilience. The goal shouldn’t be perfection, it should be good enough choices that you can sustain and don’t leave you feeling deprived and miserable.
Tracking your brain age is great way to know whether your choices are good enough to keep you on the right trajectory.
If you’ve had your genetics tested through NeuroAge, your APOE status should factor into your dietary strategy. If you haven’t, and brain health is important to you, knowing your genotype is one of the most actionable pieces of information you can have.
As always, I’m working on this for myself too. I’ll keep you posted on what I find.

Written by
Dr. Christin Glorioso, MD PhD
Dr. Glorioso is the founder and CEO of NeuroAge Therapeutics. With her background in neuroscience and medicine, she is dedicated to revolutionizing brain health and helping people maintain cognitive vitality.
Learn more about Dr. Glorioso

