
Hormone Replacement Therapy (HRT) and the brain
What starting HRT taught me about the role of estrogen and progesterone in sleep, energy, and mood
Hormone Replacement Therapy (HRT) has changed my life for the better. It has fixed my sleep, improved my mood, and improved my energy. As a neuroscientist, it has also taught me some interesting things about the role of estrogen and progesterone in our biology.
My HRT journey started in 2022, when I was 41, with me tracking, well a lot of things, but one of them was my mood. I was using a little kid-style sticker system on my wall calendar. You can see a pretty typical month of tracking below. Many of the behaviors that I track are questions that are now in the NeuroAge Sunday Survey, which will eventually become an app.
The start of my menstrual cycles are the pink dots on the 1st and 28th of the month in the upper right hand corner. Above that dot is my mood score for each day, color coded in shades of green. Forrest green is a typical happy day- 7/10 mood for me. Lighter leaf green is a 6/10, a sadder day for me, and brownish-green is a fairly hard day for me or 5/10 mood. You can see a pattern of a pretty happy first half of the month and then about halfway through there are a few hard days, a rise back to normal, and then another few hard days.
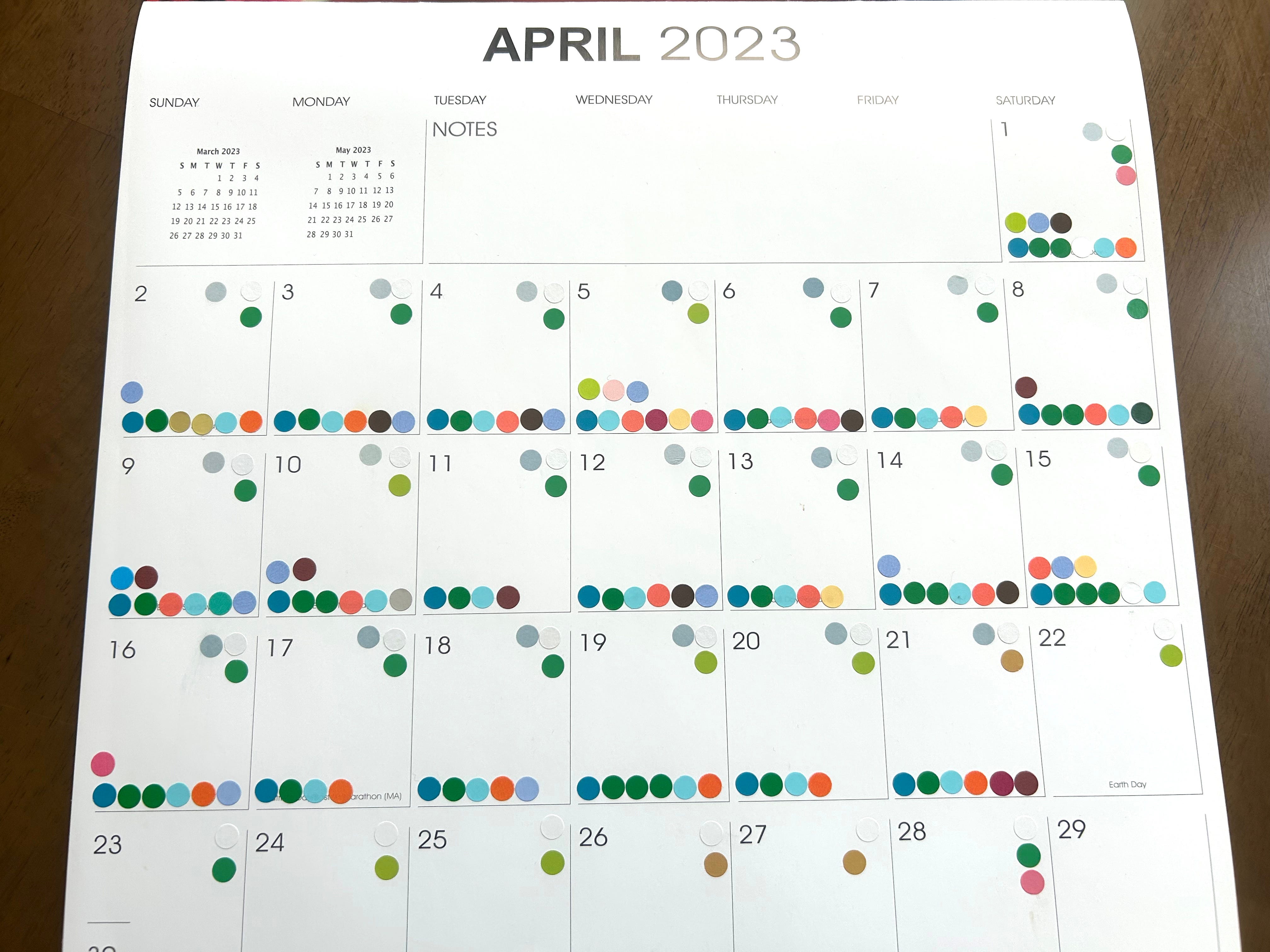
I tracked this for about two years and this pattern held every month. Of course other things could tank or elevate my mood— things going well or poorly with the business, for example, but mostly my mood held steady with this monthly pattern. I knew about pre-menstrual syndrome so having a few hard days right before my period was something that I expected but I did not expect the few hard days in the middle of the month. My lack of awareness of this pattern and why it occurs now seems astonishing to me given that I am a physician and neuroscientist.
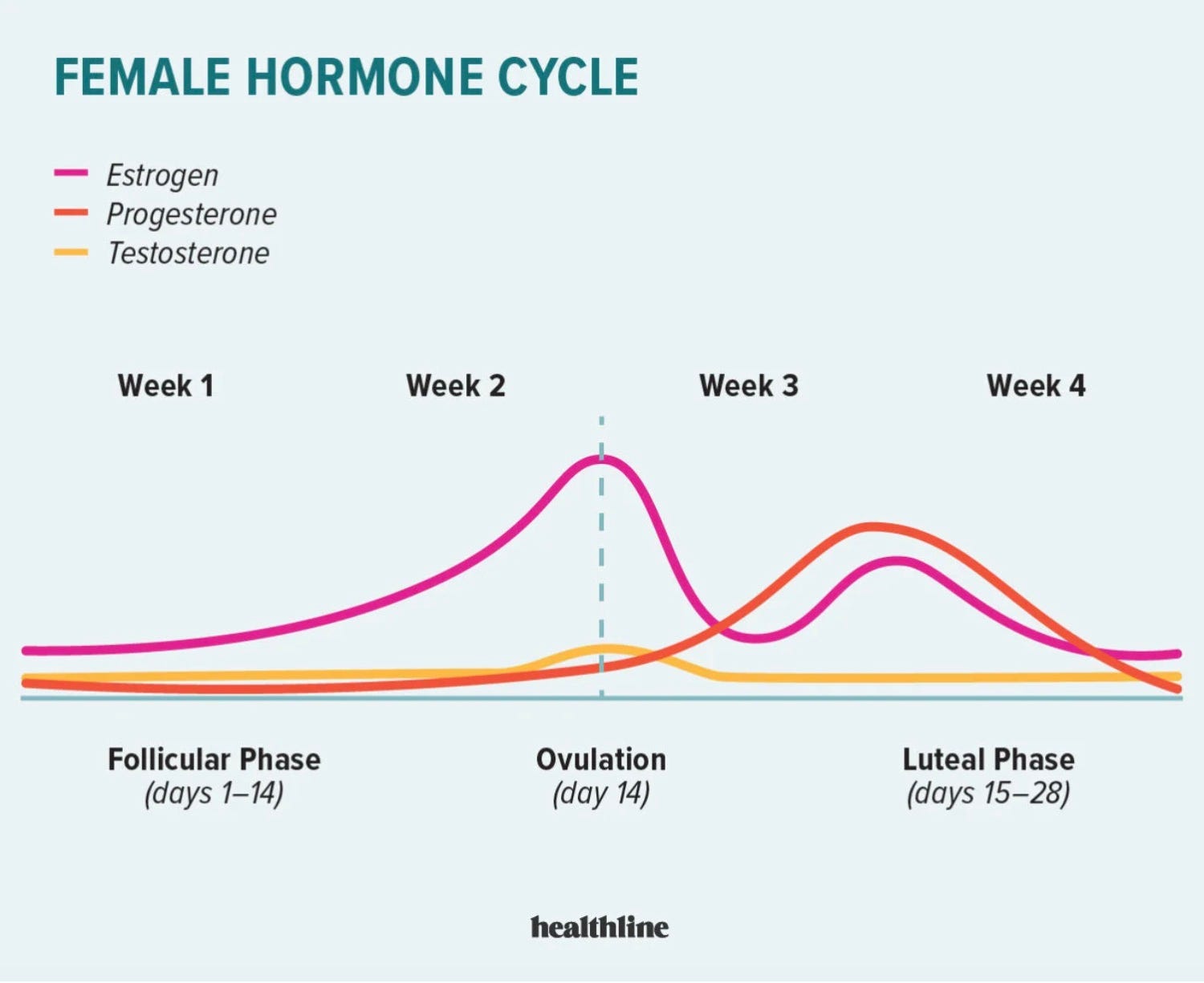
To figure out exactly why this mood pattern might be happening I googled the hormone chart in the menstrual cycle— example below. What you can see is that the days that my mood dips perfectly map onto the days that my estrogen dips (pink line below).
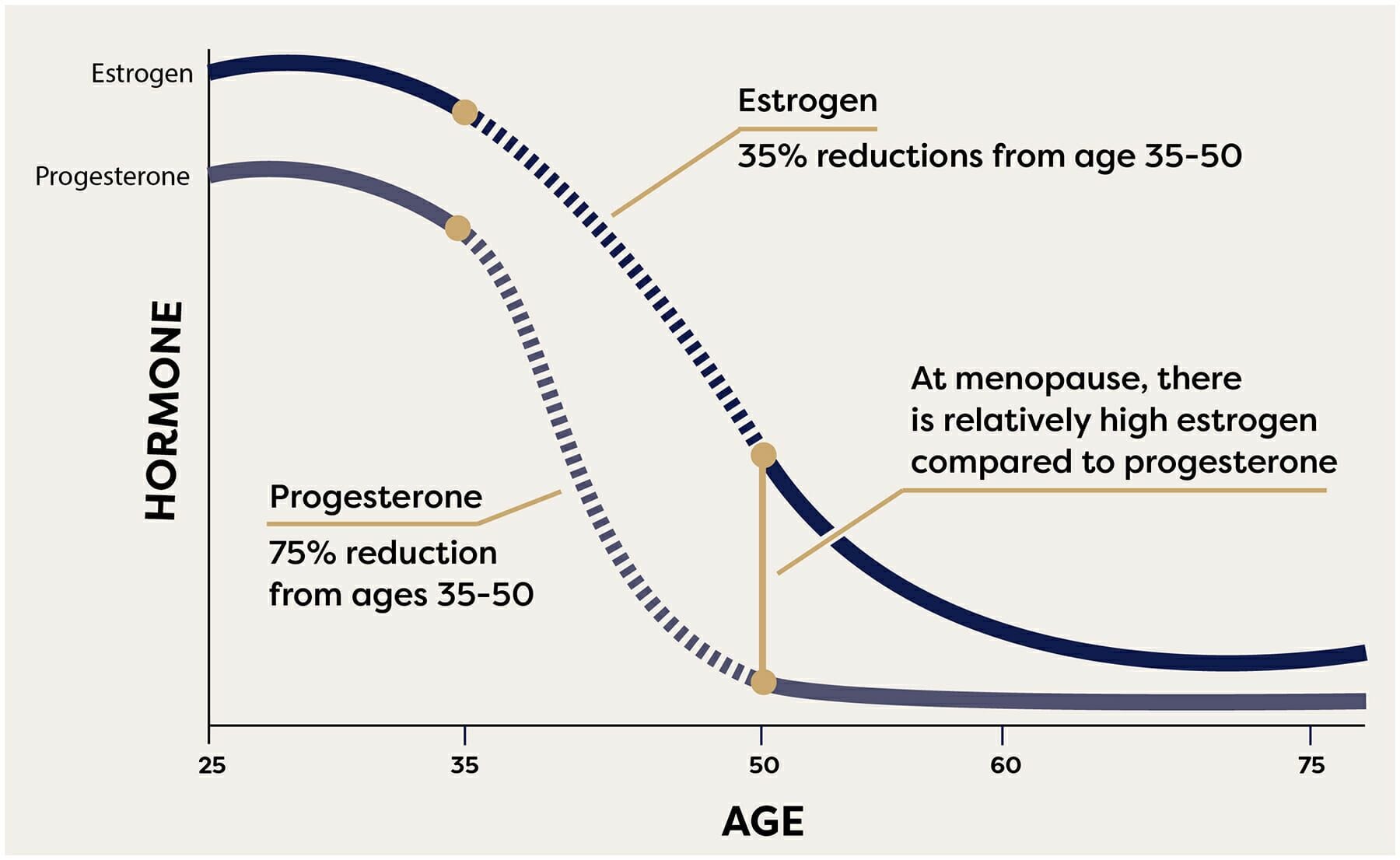
Around my late 30s/early 40s, my sleep started to become disrupted. I would wake up at 3 or 4 am and not be able to get back to sleep 3, 4, or even 5 times/week. After tossing and turning and ruminating unhappily for a couple of hours, I would finally get up and feel exhausted that day. I assumed that this was due to stress. Certainly the night before a big day, like giving a talk in front of a lot of people, I usually don’t sleep well; and being an entrepreneur is full of big days. However, another thing known to disrupt sleep is perimenopause and my sleep issues corresponded with the expected timing of age-related changes in levels of female hormones— see below.
Symptoms of perimenopause (fun times):
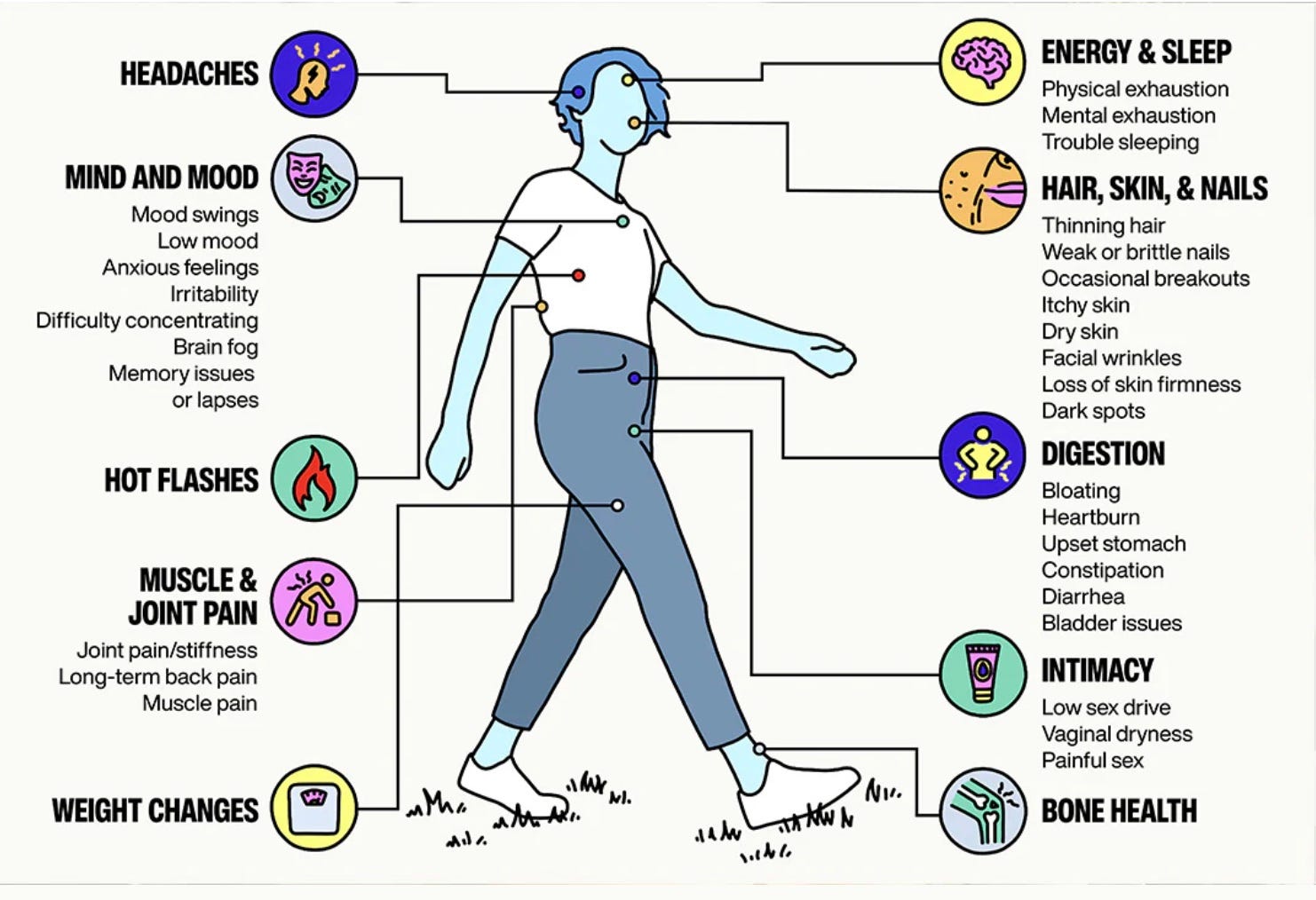
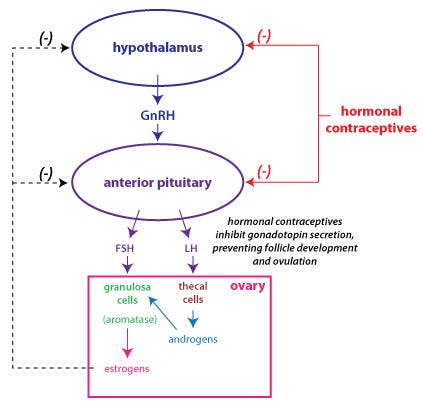
I also had the occasional hot flash and noticed some other symptoms that could be consistent with perimenopause. So I asked my PCP to try Hormone Replacement Therapy. She instead prescribed me hormonal birth control, which is NOT the same thing. Birth control pills have high dose synthetic estrogen plus progestin that “tricks” your body into not ovulating.
HRT on the other hand has bioidentical hormones at lower levels that won’t prevent pregnancy. I humored her and gave the birth control pills a try for about a week. I had never been on OCPs before and I felt awful. It’s hard to describe what I felt like— it was some combination of intensity and anxiety, like a buzzing in my head. I really am not sure why pretty much every woman that I know in their 40s that has asked their doctor for HRT has instead been given birth control pills except that it must be some paternalism in the health care system, trying to ensure that women won’t become pregnant. Birth control is really pushed by doctors in general. This is combined with physician fear surrounding HRT left over from a Women’s Health Initiative study from 20 years ago.
Realizing that my PCP was not going to be helpful, I googled how to get an HRT prescription and found the online women’s telehealth platform, Midi. I was reassured that they were prescribing FDA-regulated bioidentical hormones and took my health insurance. I have no affiliation with Midi except that I love them. I have had a really positive experience under their care.
The Midi nurse that I video chat with once a month now asked me about my symptoms of perimenopause and sent a prescription into my pharmacy for HRT. It was super simple. She started me on a very low dose of estrogen- 0.025 mg/day patch and 50 mg/day progesterone pill at night. I immediately felt an elevation in my mood and started sleeping better. The patch was supposed to be changed about every 4 days but I was noticing that I started having a drop in mood on day 2. My sleep also wasn’t perfect. She ramped up the patch dose to 0.075 mg/day and the progesterone to 100 mg/day. I now only wake up at 3 am once or twice a month. It fixed my sleep. Progesterone is a mild sedative, which is why you take it at bed time.
The estrogen makes me feel great. Really great. It even smoothed out the low mood points in my normal cycle. I feel more energetic and my hair is returning to its silkier former self. The one downside is that I did end up with an allergic skin reaction to the glue in the patches but this was easily solved by switching to a daily gel form of the estrogen.
So how does this relate to preventing Alzheimer’s? Alzheimer’s is 2X as common in women than men and we don’t yet know why this is. We know that sleeping poorly and depression are both associated with increased Alzheimer’s risk and hormone drop during perimenopause exacerbates both of those. Newer meta-analysis data shows up to a 32% reduction in Alzheimer’s risk with HRT but only if started +/- 10 years of menopause. If HRT is started in women >65 years, there is actually an increased risk of Alzheimer’s.
From that meta-analysis:
”Collectively, the most robust finding in our study was that ET initiated in midlife, likely in response to menopausal symptoms, had moderate positive effects on AD risk reduction. These data provide statistical integration of prior evidence of positive effects of ET (Yaffe et al., 1998; Hogervorst et al., 2000; LeBlanc et al., 2001; Song Y. J. et al., 2020; Zhang et al., 2021) or of midlife use (Yaffe et al., 1998; Hogervorst et al., 2000; LeBlanc et al., 2001; Wu et al., 2020). Additionally, a longer duration of use was associated with protective effects, in agreement with some previous reports (Hogervorst et al., 2000; Wu et al., 2020). This is clinically relevant as cohort studies have reported an almost doubled long-term risk of dementia with surgical menopause (Rocca et al., 2007, 2014; Phung et al., 2010; Bove et al., 2014).”
If better sleep, more energy, lifted mood, and silkier hair isn’t enough reason to start HRT in perimenopause, reducing your risk of later Alzheimer’s should be.

Written by
Dr. Christin Glorioso, MD PhD
Dr. Glorioso is the founder and CEO of NeuroAge Therapeutics. With her background in neuroscience and medicine, she is dedicated to revolutionizing brain health and helping people maintain cognitive vitality.
Learn more about Dr. Glorioso

