
Are GLP-1RAs the first longevity drugs?
What we know so far from the scientific literature
Disclaimer: this Substack shouldn’t be taken as official medical advice. I recommend that you speak with your doctor about any prescription medication changes.
Scientists and clinicians in the longevity field have been waiting for the first “longevity drug” to become available. They have differing definitions of what a longevity drug actually is. For me, it means a drug that prevents or treats multiple age-related diseases and extends both healthspan and lifespan. Some people in the field would add that a longevity drug must extend lifespan and healthspan in people without any diseases. ~95% of people in the US over the age of 65 have at least one chronic age-related condition and ~80% have two or more. So while I wouldn’t say that aging is a disease, I would say that it’s very unlikely that you will be able to grow old without having any diseases. Put another way, many age-related diseases are an extension of the normal aging process. Plaque in your arteries, blood pressure, and fasting glucose levels rise steadily with age starting in your twenties on average. In the brain, neurons die in certain regions and the connections between neurons become more sparse. With enough time, these age-related disease risk factors cause a heart attack, diabetes, or a neurodegenerative disease. Those risk factors, however, are affecting quality of life for people long before they are diagnosed with a disease. Having clogged arteries or dying neurons, can cause you to feel less fit, or be less cognitively sharp, even if a physician would not diagnose you with having heart disease or a neurodegenerative disease. Requiring a drug to demonstrate benefits in disease-free individuals before calling it a ‘longevity drug’ is unnecessary.
With some caveats and still open questions, GLP-1 therapeutics (Ozempic and Wegovy), do seem to be meeting my definition of a longevity drug. A paper that came out in Nature Medicine last week illustrates the broad protective effects of GLP-1s against age-related diseases. The blue dots in the below figure are diseases that are less prevalent in people with diabetes treated with GLP-1RAs compared to matched diabetics on other diabetes medications.

Why compare diabetics on GLP-1RAs to diabetics on other medications? Because presumably their diabetes is being treated equally well on other medications, so this helps to tease apart what is an effect of GLP-1RAs vs. what is an effect of simply having better diabetic control.
Less prevalent diseases in people taking GLP-1RAs include cardiovascular disease, IBD, drug and alcohol disorders, mental health disorders, neurodegenerative diseases, and some infectious diseases. In orange dots are the diseases that are more prevalent in people prescribed GLP-1RAs. The increase in prevalence of GI-related conditions such as GERD and gastritis are not surprising given that GLP-1RAs cause delayed stomach emptying and nausea in some people. The increase in some arthritis-related and kidney disorders are somewhat surprising to me and should be taken into consideration for people who have a predilection to these conditions. Many of the conditions in orange may lessen over time as is commonly seen with GLP-1RAs or be mitigated by lower dosing.
Are GLP-1RAs helpful in people without disease?
Whether it would be a net benefit to healthspan to take these drugs in normal weight and non pre-diabetic/diabetic people is an open and very interesting question. At the heart of that question is whether GLP-1 drugs are having benefit through weight loss and blood sugar regulation alone or if there are additional anti-aging properties of these drugs that would be beneficial in the absence of disease. Another open question is whether blood glucose stabilization in people who are not diabetic/pre-diabetic is beneficial to health and lifespan. Additional clinical studies will need to be conducted to answer these questions but for now let’s take a look at what we know so far.
How do GLP-1RAs work?
GLP-1 is a circulating peptide hormone produced by your intestine, pancreas (the organ that makes insulin), and neurons. GLP-1RAs are synthetic versions of this protein that are modified to degrade less easily and stick around in your circulation for longer than the GLP-1 that your body makes. GLP-1 has effects on many different cell types in your body including cells in your gut, pancreas, vascular smooth muscle cells that line your arteries, and your neurons.

GLP-1 works through known longevity pathways
One reason to suspect that GLP-1RAs might be longevity drugs is that they work, in part, through known longevity pathways. Researchers have identified the genes responsible for lifespan in animals through research starting in the 1970s and 1980s. One of the first genes identified to extend lifespan in worms (discoveries from the labs of Thomas Johnson and Cynthia Kenyon), is the Age-1 gene. The worm Age-1 gene is known as phosphoinositide 3-kinase (PI3K) in humans and is activated by GLP-1. Other known longevity-related genes that are regulated by GLP-1 include FOXO, MTORC1, and the NF-κB pathway.
GLP-1 protects cells from dying
Another reason to suspect that GLP-1RAs might be longevity drugs is their promotion of cell survival. GLP-1 not only can enhance insulin secretion from the pancreas, but also protects cells in the pancreas from dying. Cell death in the pancreas is a major cause for the onset of diabetes. If the cells that make insulin are no longer there, less insulin is produced. GLP-1 may also prevent neuron death (protective for Alzheimer’s, other dementias, and stroke) and cardiovascular cell death (protective for heart disease). In mice, GLP-1RAs reduce amyloid plaques, which can occur well before the onset of Alzheimer’s. If this is true in humans, it would make GLP-1RAs Alzheimer’s prevention therapeutics. Results of a phase 2b trial of liraglutide showed that the drug reduced shrinking of the brain by 50%. Given how safe GLP-1RAs appear to be, if these studies hold up, it would likely make them a mainstay of therapy for people who have a family history or genetic risk factor for Alzheimer’s.
GLP-1 is an exercise mimetic?
Levels of GLP-1 in the blood have been shown to be elevated immediately at 30 and 45 minutes after exercise. GLP-1RAs therefore are mimicking one effect of exercising.
Does lowering blood glucose extend lifespan in people without diabetes?
This question is essential to understand whether stabilizing blood glucose levels through GLP-1RAs would be expected to be beneficial in people who are not pre-diabetic. There is some evidence to support this. Fasting blood glucose goes up with age starting in your twenties.
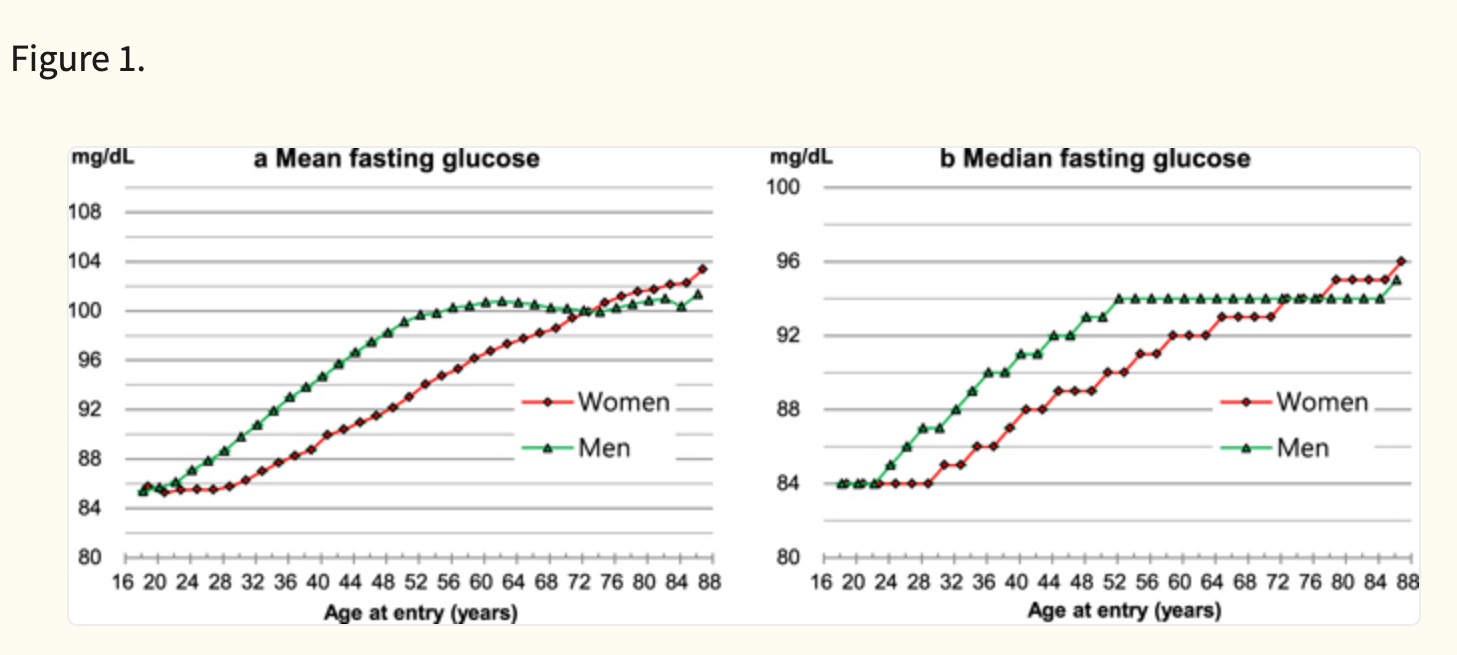
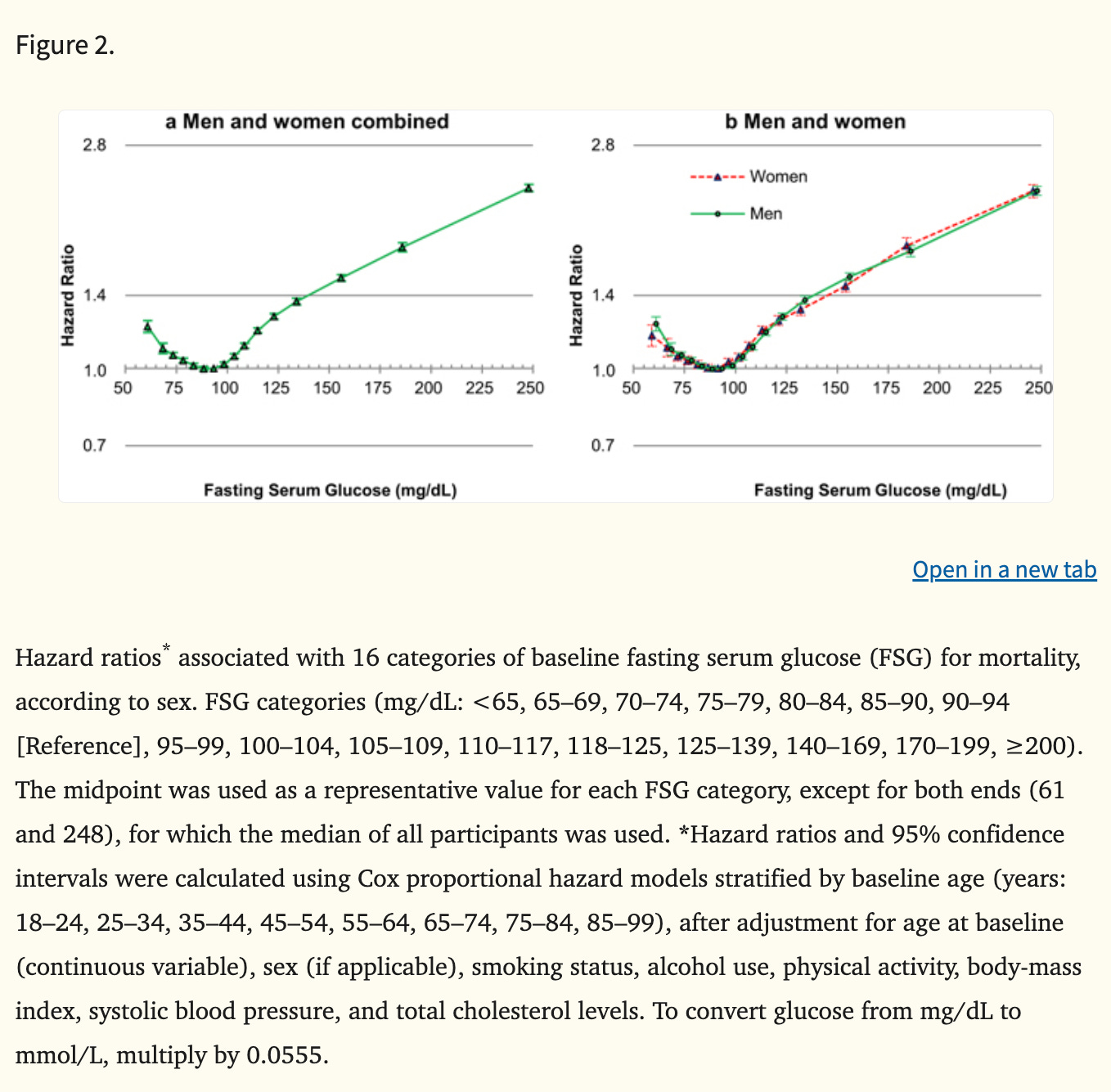
The optimal range of blood glucose for mortality is 80-94 mg/dL (see figure below). The average man has a fasting glucose of >94 starting in his late 30s according to a study. And the average woman has a fasting glucose of >94 starting around age 50. Fasting glucose levels >120 are considered diabetic, so these age-related increases in glucose do not meet criteria for diagnosing diabetes.
This tells us that the average person might want to start controlling their blood sugar around age 35-50 years old even if they aren’t pre-diabetic. Adding to the evidence, centenarians who wore continuous glucose monitors showed relatively low variability in their blood glucose levels suggesting a benefit in old age to tight glucose control.
What about people who already have optimal blood glucose levels and variability? Would GLP-1RAs be helpful to prevent their glucose levels from increasing in the future? We will need clinical trials to answer that question but there aren’t many older adults with optimal glucose levels so the pool of people who would not benefit from GLP-1RAs is narrow even without these studies.
Are GLP-1RAs beneficial for neurodegenerative diseases?
In people with diabetes, a study found that those who were only prescribed semaglutide had a 67 per cent lower risk of developing Alzheimer’s during the three-year study period than those who were only taking insulin. While there may be caveats, this points to Alzheimer’s prevention occurring not just because of diabetes management, but also because of additional protective mechanisms of semaglutide.
Results from two later-stage clinical trials are due to finish at the end of 2025 – Each includes roughly 1800 people with early Alzheimer’s who will have received either a daily tablet of semaglutide or a placebo for three years. Semaglutide is safer than the amyloid antibody therapies that were just approved for Alzheimer’s, which have the side effect of brain bleeding or swelling in ~20% of people. If semaglutide works as well or better than the amyloid antibody therapeutics, it may entirely replace them or be used in conjunction with them. We also will need clinical studies to show if anti-amyloid therapies and GLP-1RAs have additive effects and would be better in combination for treating Alzheimer’s and MCI than either alone.
Summary
In conclusion, GLP-1RAs are associated with decreased prevalence of multiple age-related diseases including heart disease, diabetes, and Alzheimer’s in people with diabetes compared to people with diabetes treated with other medications. This tells us that they are likely not working solely through weight loss or reduction of diabetes but also through other beneficial mechanisms. Stabilizing blood glucose also likely is beneficial in people without pre-diabetes/diabetes. Adding to the evidence, GLP-1 has a mechanism that works through known longevity pathways and protects pancreatic cells, heart cells, and neurons from death. It also can remove amyloid and increase health of neurons in mice.
I am convinced that almost anyone who has an age-related condition, plus those who are just a little high in fasting glucose or have cardiovascular risk factors can benefit from GLP-1RAs. I am particularly convinced for those who are diagnosed with or at high risk for neurodegenerative disorders. People who have arthritis may want to proceed with caution or titrate their dose carefully as GLP-1RAs are associated with increased risk in a recent study. Some people may not be able to tolerate the gastro-intestinal side effects of GLP-1RAs or only be able to tolerate them at a low dose.
What else do we need to know?
It’s still an open question whether GLP-1RAs can prevent disease onset in people who have universally optimal biomarkers. Basically, should we all be taking GLP-1RAs or just most of us? We will get closer and closer to having the complete picture over time as more clinical studies finish.

Written by
Dr. Christin Glorioso, MD PhD
Dr. Glorioso is the founder and CEO of NeuroAge Therapeutics. With her background in neuroscience and medicine, she is dedicated to revolutionizing brain health and helping people maintain cognitive vitality.
Learn more about Dr. Glorioso

